Frankly, at this time, I'm not so concerned with the why but rather the effect of anxiety on Steve's Parkinson's disease progression. While anxiety is not unexpected when one receives a diagnosis, from what I've read, it is a more common symptom in PD than in say Diabetes, Rheumatoid Arthritis and Multiple Sclerosis. As a matter of fact it is a PD precursor symptom, often accompanied by pessimism. I always thought that Steve was over-thinking things and expressing them in a negative way; now I realize that this was a PD potential rearing its head when he was still a young man.
What we do know is that embarrassment is a risk factor for anxiety and social fears. We know that there might be an association with levodopa although probably not the other PD meds. We know that there may be an association with norepinephrine (dopamine is the norepinephrine precursor so you can't have one without the other) and we know that there are several other neural pathways which might contribute. We've got our eye on Serotonin and GABA.

The treatments for PD anxiety at this time are problematic. Antidepressants of various classes: Tricyclics, SSRIs, Anti-psychotics, Benzodiazepines, and non-selective MAOIs. In early 2010 we just weren't ready to risk the motor symptom treatment for the anxiety/non-motor symptom.

We recently made some other nutritional supplement changes and I adjusted up and down to determine if they constituted any part of the problem. All the time, the vivid dreams, the hallucinations and illusions increased making Steve's reality very confusing; contributing to the a high anxiety level.
We finally resorted to using an herbal to help with the anxiety after I realized that he was self-medicating with aspirin and found an empty bottle - which had been almost full a week before. I read everything I could find about the herbal components because it does help relieve the anxiety on a short term basis. The best I can say is that it seems to have the fewest contraindicated ingredients. Certainly a better option now than prescription medications.

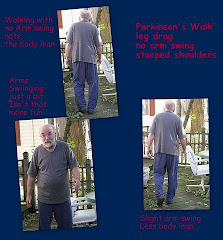
I can now see that fear in his shuffle step. It makes me wonder how many shufflers out there are just plain scared. I hadn't seen it in those movements for many months but now I recognize the enemy. It isn't just postural instability - a precursor or early symptom of his - it is his terror that something bad will happen on the next step.
I know he has recovered just enough arm swing with the new form of buffered creatine monohydrate that he can walk at a slow pace but with a normal balanced stride, shifting his weight from side to side, using his shoulders to propel himself forward (that's Walk Forward) He has to be reminded in the early morning, when he wakes from a nap and in the evening but sometimes he can let himself relax enough to walk without anxiety. That makes my heart sing.
I know he has recovered just enough arm swing with the new form of buffered creatine monohydrate that he can walk at a slow pace but with a normal balanced stride, shifting his weight from side to side, using his shoulders to propel himself forward (that's Walk Forward) He has to be reminded in the early morning, when he wakes from a nap and in the evening but sometimes he can let himself relax enough to walk without anxiety. That makes my heart sing.
 |
| Watch those stairs |

Addendum 3/12:
On 3/06/12 The Parkinson's Disease Foundation presented an Expert Briefing, A Closer Look at Anxiety and Depression in Parkinson's Disease led by Dr Laura Marsh. The archived webinar/podcast is now available at PDF. Listen rapidly as Dr Marsh covered a lot of material in a short period of time. I plan to listen again.