Can Isradipine reverse neuronal degeneration in Parkinson's?
Parkinson's is a common neurological disease, affecting over 1.5 million people in the USA alone. The risk of PD increases as we get older, especially after we pass sixty. PD progression is the result of the damage and on-going deterioration of the dopamine neurons.
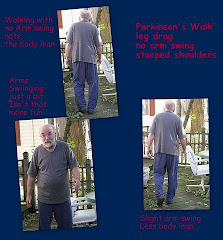
Because dopamine is a chemical messenger for the brain, the death of its neurons causes an ever increasing slow loss of motor control as it causes the typical PD symptoms: tremor, balance, loss of sense of smell, stiffness, inability to dress one's self, swallowing and speaking problems, sleeping issues, sexual dysfunction, dystonia, depression, apathy and many others.
There is a great deal of research underway but there is no cure. The only drug that has some proven neuro-protection thus far is Azilect.
Researchers understand that the neurons die but not much about how or why. While there are signs of the disease process in many regions of the brain, the core symptoms of PD occur when the dopamine neurons in an area of the brain called the substantia nigra pars compacta are damaged. Although in their youthful stage they relied upon sodium channels, as these neurons age they rely on calcuim channels to maintain autonomous activity. This reliance puts the metabolic mitocondria under sustained stress causing cell aging and death.
The calcium channels underlying the autonomous activity of the dopamine neurons are similar to the L-type channels of the heart and smooth muscles. Systemic administration of Isradipine, an L-type blocker of C type channels (Ca2+) causes a reversion to a sodium mechanism to produce independent activity.
Reversion to the sodium and HCN channels found in the juvenile substantia nigra offers protection from toxins to lab rodents with experimental PD. In a few years this could result in a Parkinson's Disease neuroprotective usage for a drug class that has been safely used by cardiac patients for decades. There is the possibility that reversing the synaptic dysfunction, neuron degeneration and reduced plasticity can restore brain cellular and molecular homeostasis; a return to normalcy.
Now there is a fresh approach to combating this disease, a different viewpoint. Isradipine Phase II clinical trials for safety and efficacy begin May 2009.
This research also suggests that although genetic and environmental factors can hasten its onset, PD is programed into all humans, if we live long enough we may all get it.
Resources:
10/06/2007
Calcium, aging and neuronal vulnerabilty in Parkinson's Disease
PUB MED NIH
D. J. Surmeier
07/05/07
Parkinson's disease: return of an old prime suspect
PUB MED NIH
D Sulzer, Y Schmitz
06/06/07
Calcium and Neurodegeneration
PUB MED NIH
MP Mattson
06/28/07
"Rejuvenation" protects neurons in mouse models of Parkinson's disease
PUB MED NIH
CS Chan, JN Guzman, E Ilijic, JN Mercer, C Rick, R Tkatch, GE Meredith, DJ Surmeier
Tuesday, February 17, 2009
9 comments:
Welcome to Parkinsons Focus Today.
We are delighted to hear from you by comment here
or through email as found in Contact Us.
Please do not include email addresses if leaving a comment online.
Email addresses are used only for email responses.
Spammers take note: your messages will not be published. The comments section is for an exchange of ideas, not for backlinks.
Subscribe to:
Post Comments (Atom)












Could this drug help Tourette Syndrome or tic disorders?
ReplyDeleteIsradipine is a calcium channel blocker and as a CA antagonist it has been studied as a medication for Tourette's Syndrome (TS) along with some beta blockers.
ReplyDeleteOne study found that Flunarizine, another CA channel blocker is supposed to be more effective.
You are on the right track.
Because both medications lower blood pressure there can be contraindications.
If effective, this type of medication would certainly be preferable to narcoleptics often taken to reduce tics. They are also prescribed for use in combination.
We will be more than happy to send you further study links if you Contact Us by email.
My doctor suggests my starting a low dosage of isadipine to counteract my stage 1 PD. My concern is that I have low blood pressure (sometimes 90/60). What would be an educated guess about a safe initial dosage?
ReplyDeleteOK, the BIG Northwestern Study is complete. What's next? Timeline for patient useage?
ReplyDeleteWhat dosages were found to be tolerable AND efficacious (i.e. in pts. with hi or low BP)?
I hate to rain on your question but I think dosage questions belong with your doctors.
DeleteThe results of the isradipine clinical trials using 5mg, 10 mg and 20 mg can be found here:
http://clinicaltrials.gov/ct2/results?term=Isradipine&recr=Closed&rslt=&type=&cond=Parkinson%27s+disease&intr=isradipine&titles=&outc=&spons=&lead=&id=&state1=NA%3AUS%3AIL&cntry1=NA%3AUS&state2=&cntry2=&state3=&cntry3=&locn=&gndr=&rcv_s=&rcv_e=&lup_s=&lup_e=
There was also a DynacircCR trial to which you can find a link here:
http://clinicaltrials.gov/ct2/show/NCT00909545?term=Isradipine&recr=Closed&cond=Parkinson%27s+disease&intr=isradipine&cntry1=NA%3AUS&state1=NA%3AUS%3AIL&rank=1
I"m sorry Anonymous from November but we cannot make an educated guess for your dosage since you already have low-normal pressure. Again, this is a medical issue which you and your doctors need to consider.
I was diagnosed in 1996 at the age of 46 with PD. I started with the standard list of drugs to block the symptoms. In Aug 2010, I started, with my neurologist's approval, my own treatment with isradipine. I started with 10 mg/day and titrated up to 40 mg/day in 8 weeks. Luckily, I have hypertension (160/100) and was able to drop the drugs I was taking for my hypertension and use the isradipine to also control my hypertension. At the 4th week, I noticed an increase in my tremors and more hesitation in my gait. At the 6th week, My symptoms gotten so bad that I almost gave up and stopped the isradipine treatment. What I decided was happening was that the Ca channel was being blocked and the Na channel had not yet opened, causing my neurons to stop producing what little dopamine that they were providing. I decided to keep trying until I reached my goal dosage. On the 8th week, I had reached my dosage goal of 40 mg/day, and I began to notice an improvement in my PD symptoms. When I was given the standard set of PD tests in Dec 2010, my neurologist said that my test scores had indicated that my PD had reverted to what it was in Dec 2009. Since 2010, I have continued to take isradipine and during that time my tremors have ceased, and the only PD symptom I have is a gait problem. My hypertension that I was having trouble maintaining before starting isradipine has become very stable at 130/60.
ReplyDeleteGary, thank you for sharing this information.
Deletegary, Do you have an update on how things are going? I am starting to take isradapine and am quite interested. Ed
ReplyDeleteThere is still a search for the proper L-channel calcium channel blocker.
DeleteYou might want to read this article from September 2014. You'll have to cut and paste the link below to read more about STEADY-PD.
http://health.ucsd.edu/news/releases/Pages/2014-09-30-phase-III-parkinsons-clinical-trial.aspx
Another article of interest is from June 16, 2013:
http://www.pdf.org/en/science_news/release/pr_1373985871
At this point no earth-shattering findings have been published.
On January 20, 2015 The National Parkinson Foundation did have a webinar to discuss STEADY-PD III but I can't locate the archives at their website.