It's been around for more than 20 years. It's always been controversial. It's had a few clinical trials, now it's getting more.
 Some say it works, some say it does nothing. A lot of people view it as another form of snake oil. But there is a community that believes it can help MS, ALS, Parkinsons, Alzheimers, Cancer, HIV/Aids, Celiac Disease, Crohns disease, Fibromyalgia, IBS and several other diseases. Warning signals go off in my head when a drug claims it can cure or slow so many serious things. But I'll ignore them and take a look at what's being claimed.
Some say it works, some say it does nothing. A lot of people view it as another form of snake oil. But there is a community that believes it can help MS, ALS, Parkinsons, Alzheimers, Cancer, HIV/Aids, Celiac Disease, Crohns disease, Fibromyalgia, IBS and several other diseases. Warning signals go off in my head when a drug claims it can cure or slow so many serious things. But I'll ignore them and take a look at what's being claimed.Here's how it is thought to work: Naltrexone is an opioid blocker, it blocks all the brain's opioid receptors and it was approved by the FDA to treat recovering addicts. The low dose version triples the body's production of endorphins which gets the immune system into full operation. The drug doesn't fight the diseases directly, the body fights the diseases after the immune system is back to normalcy.
Naltrexone is generic so no drug company will pay the millions needed to go through the off-label process with the FDA or the EU drug agency because there's no profit in doing so.
Another problem is that the drug comes in a 50mg capsule for the use of the addicts. Other human diseases would mainly use doses of 1.75 to 4.50 mg per day ("low dose" or LDN). To get capsules with the necessary dose size the patient wishing to use this drug needs to find a compounding pharmacy that is experienced with LDN. I think that some of the problems that off-label patients have had with the drug may have been inaccurate dose size from the compounding pharmacy. It is available in liquid form which must be kept refrigerated. If using the solution, you need to stipulate that you do not want the slow-release (SR) form. Remember also that you will need to titrate up to a dose effective for you. We've read of some MS patients only stop at 2.8mg and do not go all the way to 4.5mg.
 It is important to take it between 11:00pm and 3:00am because the body makes endorphins in the last few hours before sunrise. Naltrexone is an opioid blocker-opiate antagonist; it makes the brain think it has a deficit of endorphins. So to compensate the body makes 2 to 3 times the normal amount of endorphins. The endorphins function restore the immune system to full operation. Some LDN users also add chlorella to their regimen for additional support.
It is important to take it between 11:00pm and 3:00am because the body makes endorphins in the last few hours before sunrise. Naltrexone is an opioid blocker-opiate antagonist; it makes the brain think it has a deficit of endorphins. So to compensate the body makes 2 to 3 times the normal amount of endorphins. The endorphins function restore the immune system to full operation. Some LDN users also add chlorella to their regimen for additional support.Purely anectdotal evidence exists showing LDN reducing symptoms in MS patients and to a
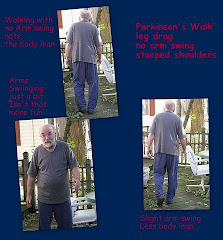
 lesser extent in Parkinson's. At a site listed below the following improvements were noted: sense of well-being; no more depression; improved sleep; episodes of delusion/paranoia stopped; ease of muscle tension followed by restored normal breathing pattern; lowered doses of PD meds; improved cognition; restoration of balance; no more night sweats; no drooling; smile returned; lack of side-effects. (1/2011 update) A recent anecdotal report indicates that tremor reduction after 6 days of use. It is too early to determine if this is due to the effects of LDN or placebo effect.
lesser extent in Parkinson's. At a site listed below the following improvements were noted: sense of well-being; no more depression; improved sleep; episodes of delusion/paranoia stopped; ease of muscle tension followed by restored normal breathing pattern; lowered doses of PD meds; improved cognition; restoration of balance; no more night sweats; no drooling; smile returned; lack of side-effects. (1/2011 update) A recent anecdotal report indicates that tremor reduction after 6 days of use. It is too early to determine if this is due to the effects of LDN or placebo effect.So how do you obtain LDN? You print out some information and you discuss it with your doctor...who might mention the connection between T-cells and decreased dopamine but not that LDN might adjust the glial process...Which we will be discussing in the future.
Clinical trial results:
http://www.ncbi.nlm.nih.gov/pubmed/17222320
http://www.lowdosenaltrexone.org/ldn_trials.htm
Parkinsonian symptom abstract
http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6T0C-4FTS37F-5&_user=10&_rdoc=1&_fmt=&_orig=search&_sort=d&view=c&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=50ee2ac9fb3795a3bb2c046b749e83ad
An interesting news item
http://www.mailtribune.com/apps/pbcs.dll/article?AID=/20080310/NEWS/803100308/-1/LIFE
You might find these interesting:
http://www.revolutionhealth.com/drugs-treatments/rating/naltrexone-for-parkinsons-disease http://www.digitalnaturopath.com/treat/T74481.html
Specifics about Low Dose Naltrexone
Check this site for LDN information
and also this one: http://www.lowdosenaltrexone.org/
Our next two posts in this series:
Low Dose Naltrexone and Parkinson's Disease III: Dosage and Timing
Although the Parkinson's LDN database at LDN World Database is small, it will provide some helpful information. If you are using LDN for PD or know someone who is, it would be a great idea to make your addition to the database. They have a much longer MS database and a list (database) of pharmacists as well.
Addendum 3/29/11
Many patients are also taking Alpha Lipoic Acid as a supplement when they take LDN. Watch for R-ALA which is the positive form.
Researchers are now looking at natlrexone to treat the inpulse-control side effects of PD meds. We are wondering if those who take Mirapex and Selegiline or other dopamine agonists or MAOIs would be able to continue to have the benefits of those medications without the problems which many PwPs have experienced.
Addendum 3/29/11
Many patients are also taking Alpha Lipoic Acid as a supplement when they take LDN. Watch for R-ALA which is the positive form.
Researchers are now looking at natlrexone to treat the inpulse-control side effects of PD meds. We are wondering if those who take Mirapex and Selegiline or other dopamine agonists or MAOIs would be able to continue to have the benefits of those medications without the problems which many PwPs have experienced.
see: Naltrexone for Impulse Control Disorders in Parkinson's disease.
Addendum 6/27/11
Because we think this is very important, we just want to remind anyone taking LDN to always have a bracelet/dogtag/pendant/wallet card indicating that you are taking Low Dose Naltrexone.
In the event of a bad fall or other injury, you don't want to be given narcotic/opiate painkillers or you will have pain far worse than the pain you are already experiencing.
It has been suggested that this tag indicate Naltrexone at the very least as some people may not be familiar with LDN.












Appreciate your balanced article.
ReplyDeleteOne thing--it appears that the dosing timing information may be outdated. http://glasgowldn2009.com/category/diary/
Thank you for sending that wonderful link. We have written an update to the update as a result of your comment.
ReplyDeletethis is a question to the parkinsons people.
ReplyDeleteThose who take mirapex for treatment,that would be just about everyone.
i am interested in the maximum daily dose that
your doctor prescribed for you.
thanks,
An above question about LDN dosage was reposted by us because there was a signature in the question while the selected name was anonymous.
ReplyDeleteWe honor that anonymous status by reposting the question without a name unless we are advised to the contrary.
To Rena, please be advised that we cannot provide a dosage instruction for LDN. Moreover, we were simply reporting about the status and not speaking from personal experience.
I believe the information you are looking for is in the 6/19/2009 article Low Dose Naltrexone and Parkinson's Disease Part III - Dosage and Timing Updates.
Thank you for visiting and we hope this helps.
You may contact us directly through the CONTACT US links throughout Parkinson's Focus Today.
Diagnosed with PD at 30, it's been four years now and I would like to try LDN. What compelling info would be good to bring to my neuro?
ReplyDeleteThanks for your article.
You might consider listing your symptoms and their frequency. Next to each indicate how they disrupt your lifestyle.
ReplyDeleteThe next thing I would suggest is a list of every medication and supplement you are currently taking - sometimes there are meds you might get from one doctor which won't appear on the you records with another. It is important that you are not on anything resembling an opiod.
We have already listed the anectdotal reports of the benefits PwPs have found with LDN so you might present the entire list with your hopes circled:
1) sense of well-being;
2) no more depression
3) improved sleep
4) episodes of delusion/paranoia stopped
5) ease of muscle tension followed
6) by restored normal breathing pattern
7) lowered doses of PD meds
8) improved cognition
9) restoration of balance
10) no more night sweats
11) no drooling -
there are other swallowing issues related
to drooling - if you have them, list them
There is a relation to speaking voice also.
12) smile returned
13) lack of side-effects
You can always print these articles and any of the links provided within them as part of your argument.
We'd love to hear how you do if you try LDN.
Hello
ReplyDeleteMy father is 86yrs of age and started taking LDN on April 18, 2011.
Can anyone tell me how long after you started taking LDN that you noticed improvement/change/benefits?
Regards
John (Australia)
Hi John, everyone is different, depends on the illness and how long you have suffered and body type/size, too many varibles. My research has been over a year, and I have read some feel it in one day, some feel it in months, you have to make sure you are getting it from a rep pharmacy to ensure you are acutally using Naltrexone in the low dose form. The ones who feel it right a way I FEEL its from the added endorphins, I was one who felt it pretty fast and I only started at 1.0 went up to 3.0 in 3 months. I had a few side effects, some tummy issues but I have IBS too, and the added endorphins help digestion and yeah I felt it. NOW MY IBS IS almost totally under control, food and stress, I take less of my ativan since Im in a better mood, i.e. added endorphins there too, I believe some of us have endorphin deficiency syndrome, I looked it up since had mood change for the better and my knee pain was helped big time in 5 days, I LOVE MY LDN and anyone wanting to use it PLEASE research it every day until you feel its for you.. no one can tell you its for you.. its a great treatment for my fibro/cfs/IBS/arthritis in my knees.. GOOD LUCK!!
ReplyDeleteLDN has two mechanisms of action: endorphins, and anti-inflammation.
ReplyDeleteParkinson's is a disease of neuro-inflammation, so the endorphin effects of LDN may be only of secondary relevance to PD.
LDN's anti-inflammatory effects are due to its blocking of the TLR4 receptors on microglia (part of the immune system in the brain). These receptors are activated by the alphasynuclein that is released from dopaminergic neurons when they are damaged. Alphasynuclein stimulating TLR4 causes microglia to get into a highly activated state in which they produce pro-inflammatory cytokines such as would be used to attack an invading pathogen. This kind of response can damage undamaged "bystander" neurons, causing those erstwhile healthy neurons to release more alphasynuclein into the inter-neuron environment, thus re-stimulating the TLR4 receptors and causing the microglia to continue their damaging attacks.
Normally, microglia have a more low-key response to cells breaking down, which involves cleaning up the debris without damaging healthy bystander neurons. But the TLR4 receptor is the same receptor as it stimulated by pathogens like staph infections, and so the fact that alphsynuclein stimulates TLR4 makes the microglia respond as if an invasive microorganism were present, and that is what sets off the autoimmune cycle.
The hope is that LDN, by blocking TLR4 for 3-4 hours per day, will give the microglia time to calm down and not get revved up into a highly activated state. But I'm not sure how much time it really takes for them to get revved up. So if 20 hours between LDN doses is sufficient to get their activated, then LDN might not work. Otherwise, it might work.
Unfortunately, alphasynuclein / TLR4 is not the only pathway to autoimmune looping. There is also the neuromelanin that is released from damaged dopaminergic neurons. Neuromelanin is specific to the substantia nigra, and so represents a special autoimmune hazard that can lead to PD.
Neuromelanin works through another receptor called TLR2 (along with NOD2 and CD14). These receptors are not blocked by LDN. However, they are partially blocked by curcumin.
So I came up with an idea that is completely untried thus far: why not dose on curcumin at the same time as LDN? Both stay active for about 3 hours. If you could block both pathways at once, you might have a better chance of calming the microglia and interrupting the autoimmune cycle.
This is just an idea; I have no background in this area but have been reading a lot. It should be noted that curcumin is almost useless unless it is taken with Bioperine, a black pepper extract that enhances absorption by as much as 20 times. You can find curcumin products that have Bioperine added.
This is a very complicated illness and so the above is just something I came up with on my own, and we have just started to try it a few days ago, with no dramatic results so far. Something for you to think about and research further on your own. Don't do this just because I sound like I know what I'm talking about, because believe me I'm still learning about this entire area.
My guess is that you're using Doctor's Best Curcumin. Consider adding their Phosphatidyl Serine to the mix. This is also the best time to add Vitamin D3 since they work well together.
DeleteFound this article on low-dose naloxone (very close cousin of naltrexone) which explains how it can be effective against inflammation via a non-endorphin-related means of action, even at the extremely low levels which result from LDN style dosing. Note that the other path for inhibiting microglial activation, which goes through TLR4 receptors of microglia, would seem to require more naltrexone than is supplied by an LDN dose, but this path, which goes through the PHOX subunit of microglial NOX2, does respond to levels in the LDN dosing range.
ReplyDeletehttp://www.jneuroinflammation.com/content/9/1/32
Have a look at the following:
DeleteFrom 1991 Naloxone reverses L-dopa induced overstimulation effects in a Parkinson's disease animal model analogue - http://www.ncbi.nlm.nih.gov/pubmed/1900558
I've skipped the next several to jump to a completed 2011 European study which uses Oxycodone/Naloxone Prolonged Release tablets and was completed recently although there are no posted results.
https://clinicaltrials.gov/ct2/show/NCT01439100