What Is Spinal Cord Stimulation?
Spinal cord stimulation (SCS) for pain reduction has been around since 1967. How it works is actually a little more complicated that in might seem now that there are almost 50,000 of these surgical procedures performed around the world every year. The purpose of SCS is activation of neurons, making them positive electrically or depolarized so that they can generate action potential.
Theoretically pain messages are sent when the "gate" in the spinal cord dorsal horn is opened and there are more small rather than large diameter fibers active. In SCS it was found that electrical stimulation of peripheral nerves can reduce pain by activating the large diameter gated fibers in the dorsal horn of the spine. It is the opening of the large fiber gates and closing of the small gate which is supposed to prevent the pain signals from reaching the brain.
There are more mechanisms at work such as stimulation at higher frequencies causing the nerve fibers to fail to conduct the action potentials, the inhibition of impulse transmission in the spinothalamic tract and an increase of serontonin, adenosine, GABA and Substance P with a decrase in glutamate and aspartate in the dorsal horn of the spinal cord.
The procedure is to insert the epidural leads and test for 3 to 21 days. If the treatment works a pacemaker-sized generator is implanted and the external remote is provided. The procedure is not a cure of the problems at the root of the pain, the treatment is to reduce the level of pain as it threatens quality of life. Nor does the procedure work for all types of pain.
The use of SCS technology is expanding. One of the most recent areas of focus is Parkinson's disease. At Duke University in North Carolina Dr Miguel Nicolelis, Professor of Neuroscience is investigating using the spinal cord rather than the brain to treat PD symptoms because the spinal cord is the primary pathway by which the body signals the brain and the brain sends signals to the body.
In the lab rodents with induced PD, the scientists found that within 3.5 seconds of getting electrical stimulation the stiff, slow movements became essentially normal. The team experimented with higher and lower levels of electrical stimulation and with a combination of L-Dopa. What they found was that even without levadopa the animals were 26 times more active. When they received two doses of levadopa their ability to move was similar to receiving five doses without stimulation.
Since it is known that eventually L-Dopa will not only cease to work but may exaccerbate symptoms, the modified SCS should enable a serious reduction of meds if successful for the patient.
Dr Nicolelis realized that the brain activity of mice with induced PD was similar to the low frequency oscillations of rodents with seizures and epilepsy which he had previously studied. Furthermore it is felt that these low frequency corticalstriatal oscillations impair motor function so that with electrical stimulation, the activity of the neurons could be normalized and motor function could be restored.
The Duke group is working with a team from Brazil to perform pretrial testing of their device.
references and reading:
"Spinal Cord Stimulation Restores Locomotion in Animal Models of Parkinson's Disease."Romulo Fuentes, Per Petersson, William B. Siesser, Marc G. Caron, and Miguel A. L. Nicolelis.Science 20 March 2009 323: 1578-1582.DOI: 10.1126/science.1164901
http://www.sciencemag.org/cgi/content/abstract/sci;323/5921/1578
Dr Nicolelis has also worked on brain-machine interfaces:
http://www.guardian.co.uk/science/2009/mar/19/parkinsons-disease-spinal-implant-electrical-stimulation
Monday, March 30, 2009
Sunday, March 29, 2009
Rambling Thoughts
On taking a walk with Parkinson's Disease this Spring day
It's spring time here in Northeast Ohio. The maple trees are bursting with energy that's coming up from their roots. Soon seed packets from these trees will be falling into the neighboring yards up and down the street. Perhaps I could walk there but my PD stiffness and my knee hold me back. Is this season my last chance---ever?
The maple trees are bursting with energy that's coming up from their roots. Soon seed packets from these trees will be falling into the neighboring yards up and down the street. Perhaps I could walk there but my PD stiffness and my knee hold me back. Is this season my last chance---ever?
The maple trees concentrate on dropping those seeds just as soon as spring arrives because they are programed to get the next generation going before they do anything else. My new growth has been returning to a disciplined exercise regimen after more years than I care to acknowledge. It's been eight years since I used to bicycle for miles through the local parks but that was somehow different because my body cooperated, the scenery was beautiful, and I could create my own uphill and downhill challenges as I rode with the wind and sun. Maybe when it's warmer I'll take a look at the old bike, pump up the tires and see what where we can go together.
Now I sit sometimes at the physical therapy center wondering if my fellow senior patients are ever going to stop their exercise routine, if they will learn to do the exercises correctly and will they start getting better. Possibly or possibly not, but many of them can walk better than I can.
 I've had Parkinson's for 6 years now. My left knee is affected by PD stiffness and arthritis. It's very painful. That's why I've been walking with a cane to support my left knee for a few years. Lately I've been working out on Nautilus machines 5 days a week and to help my knee, I've started taking glucosamine and chondroitin again. I've been feeling better, I can touch type a little bit again and I just walked, not as far as I can see but half as far, which is great for me! The scary part is that on the two days of the week that I can't go to the exercise center, I miss it and wish I could. How has something I resisted become a love?
I've had Parkinson's for 6 years now. My left knee is affected by PD stiffness and arthritis. It's very painful. That's why I've been walking with a cane to support my left knee for a few years. Lately I've been working out on Nautilus machines 5 days a week and to help my knee, I've started taking glucosamine and chondroitin again. I've been feeling better, I can touch type a little bit again and I just walked, not as far as I can see but half as far, which is great for me! The scary part is that on the two days of the week that I can't go to the exercise center, I miss it and wish I could. How has something I resisted become a love?
It's spring time here in Northeast Ohio.
 The maple trees are bursting with energy that's coming up from their roots. Soon seed packets from these trees will be falling into the neighboring yards up and down the street. Perhaps I could walk there but my PD stiffness and my knee hold me back. Is this season my last chance---ever?
The maple trees are bursting with energy that's coming up from their roots. Soon seed packets from these trees will be falling into the neighboring yards up and down the street. Perhaps I could walk there but my PD stiffness and my knee hold me back. Is this season my last chance---ever?The maple trees concentrate on dropping those seeds just as soon as spring arrives because they are programed to get the next generation going before they do anything else. My new growth has been returning to a disciplined exercise regimen after more years than I care to acknowledge. It's been eight years since I used to bicycle for miles through the local parks but that was somehow different because my body cooperated, the scenery was beautiful, and I could create my own uphill and downhill challenges as I rode with the wind and sun. Maybe when it's warmer I'll take a look at the old bike, pump up the tires and see what where we can go together.
Now I sit sometimes at the physical therapy center wondering if my fellow senior patients are ever going to stop their exercise routine, if they will learn to do the exercises correctly and will they start getting better. Possibly or possibly not, but many of them can walk better than I can.
 I've had Parkinson's for 6 years now. My left knee is affected by PD stiffness and arthritis. It's very painful. That's why I've been walking with a cane to support my left knee for a few years. Lately I've been working out on Nautilus machines 5 days a week and to help my knee, I've started taking glucosamine and chondroitin again. I've been feeling better, I can touch type a little bit again and I just walked, not as far as I can see but half as far, which is great for me! The scary part is that on the two days of the week that I can't go to the exercise center, I miss it and wish I could. How has something I resisted become a love?
I've had Parkinson's for 6 years now. My left knee is affected by PD stiffness and arthritis. It's very painful. That's why I've been walking with a cane to support my left knee for a few years. Lately I've been working out on Nautilus machines 5 days a week and to help my knee, I've started taking glucosamine and chondroitin again. I've been feeling better, I can touch type a little bit again and I just walked, not as far as I can see but half as far, which is great for me! The scary part is that on the two days of the week that I can't go to the exercise center, I miss it and wish I could. How has something I resisted become a love?Thursday, March 26, 2009
Parkinson's Blue Light District
Optogenics and the G-protein coupled receptor - what will it mean for PD?
 It all begins in the brain, that complicated computer which processes analyzes, sorts, stores, and relays electrical impulses to keep the body functioning as designed. Sometimes, however, things go wrong, small parts malfunction, current varies to affect operation and the body human begins to get error messages. On many occasions we reboot, clean up some programs, add a program and we're good to go. Or we call IT or MIS and those specialists can fix many problems. But at other times the error messages persist.
It all begins in the brain, that complicated computer which processes analyzes, sorts, stores, and relays electrical impulses to keep the body functioning as designed. Sometimes, however, things go wrong, small parts malfunction, current varies to affect operation and the body human begins to get error messages. On many occasions we reboot, clean up some programs, add a program and we're good to go. Or we call IT or MIS and those specialists can fix many problems. But at other times the error messages persist.
Parkinson's disease sends some of those errors messages. The specialists here have been able to take patients to the edge of state of the art with medications which abate progression, which go to the source to make some symptoms ease or stop for awhile, but the disease remains. New treatments were developed to control the symptoms by interrupting the error messages. From radical surgery to invasive but less radical surgery, some patients have found relief while others were the same or worse.
We already know that not all PD patients are eligible for Deep Brain Stimulation (DBS) and that it appears to be effective for some but not all of the people who do receive the treatment. Ongoing research in an area called optogenics may become a way to change some of that situation by employing a method which allows for more precision in the surgical procedure by prior identification of the neurons which would benefit from stimulation. Basically the focus become tighter and more accurate before the nodes are set. One goal is to improve the results of DBS.
While aspects of the area of science now called Optogenics have existed for several years, the older apects are now being combined with a method developed in Karl Deisseroth's lab. By inserting a small fiberoptic cable into the brain the light impulses can be controlled as they search for the affected neurons. This procedure allows for smaller and smaller targets of the G-protein on the specific neuron.
have existed for several years, the older apects are now being combined with a method developed in Karl Deisseroth's lab. By inserting a small fiberoptic cable into the brain the light impulses can be controlled as they search for the affected neurons. This procedure allows for smaller and smaller targets of the G-protein on the specific neuron.
The current procedures were developed by under the direction of Karl Deisseroth, MD, PhD at Stanford University. The project required the work of bioengineering and medical neuroscience and neurology students and faculty as they explored target after target to finally find that stimulation of the axons that connect the subthalmic nucleus are actually in areas closer to the brain's surface. While treatments would be still invasive, they would be less invasive thanks to better targeting at the G protein coupled receptors at the cell surface.
 At Stanford University scientists were able to incorporate the technique in model mouse brains to produce activity in a real-time frame using both blue light to signal activity and yellow light to stop. The cells returned to their normal status unchanged at completion.
At Stanford University scientists were able to incorporate the technique in model mouse brains to produce activity in a real-time frame using both blue light to signal activity and yellow light to stop. The cells returned to their normal status unchanged at completion.
An interesting thing about neurons is that they communicate in a manner similar to binary code. Sometimes on sometimes off similar to the 0s and 1s of binary code. By being able to communicate in their on-off patterns, learning the neuron language might enable direct actual neural instruction through the flashing of the blue and yellow lights. In another metaphor, Optogenics appears to be the cell tower, now what is needed is a phonebook.
Optogenics holds hope for spinal cord injuries, restoring function to paralyzed limbs, allowing for new therapies, closely targeted pharmaecuticals and possibly become a neuronal therapy in itself.
Optogenics: A process by which brain cells can be activated by specific light
Channel Rhodopsins (ChR): light-activated ion channels appear to be coupled with the photoreceptor so that they do not require chemical signalling but instead are triggered by light.
Channel Rhodopsin (ChR2): algae-derived gene protein which makes neurons more active upon blue light exposure. Currently vector-introduced to the desired neurons. This is the "emit a signal" protein
Halo-rhodopsin (NpHR): from a microbe which can make neurons less active. The instruction here is to "stop emitting." They respond to yellow light.
G protein coupled receptors (GPCRs): signalling proteins found on the surface of nearly all cells.
Reading List:
http://storybank.stanford.edu/stories/controlling-brain-with-optogenics
http://www.newscientist.com/article/dn16807
http://www.freepatentsonline.com/7488583.html
http://pubs.acs.org/cen/science/86/8612sci1.html
http://www2.hu-berlin.de/biologie/expbp/Homepage-new_10408.pdf
http://web.mit.edu/newsoffice/2007/brain-block.html
http://med.stanford.edu/news_releases/2009/march/deisseroth.html
http://storybank.stanford.edu/stories/neural-traffic-light-a-go-better-brain-research
http://www.medicalnewstoday.com/articles/143132.php
Targeting the Brain's GO pathway - 2010 It all begins in the brain, that complicated computer which processes analyzes, sorts, stores, and relays electrical impulses to keep the body functioning as designed. Sometimes, however, things go wrong, small parts malfunction, current varies to affect operation and the body human begins to get error messages. On many occasions we reboot, clean up some programs, add a program and we're good to go. Or we call IT or MIS and those specialists can fix many problems. But at other times the error messages persist.
It all begins in the brain, that complicated computer which processes analyzes, sorts, stores, and relays electrical impulses to keep the body functioning as designed. Sometimes, however, things go wrong, small parts malfunction, current varies to affect operation and the body human begins to get error messages. On many occasions we reboot, clean up some programs, add a program and we're good to go. Or we call IT or MIS and those specialists can fix many problems. But at other times the error messages persist.Parkinson's disease sends some of those errors messages. The specialists here have been able to take patients to the edge of state of the art with medications which abate progression, which go to the source to make some symptoms ease or stop for awhile, but the disease remains. New treatments were developed to control the symptoms by interrupting the error messages. From radical surgery to invasive but less radical surgery, some patients have found relief while others were the same or worse.
We already know that not all PD patients are eligible for Deep Brain Stimulation (DBS) and that it appears to be effective for some but not all of the people who do receive the treatment. Ongoing research in an area called optogenics may become a way to change some of that situation by employing a method which allows for more precision in the surgical procedure by prior identification of the neurons which would benefit from stimulation. Basically the focus become tighter and more accurate before the nodes are set. One goal is to improve the results of DBS.
While aspects of the area of science now called Optogenics
 have existed for several years, the older apects are now being combined with a method developed in Karl Deisseroth's lab. By inserting a small fiberoptic cable into the brain the light impulses can be controlled as they search for the affected neurons. This procedure allows for smaller and smaller targets of the G-protein on the specific neuron.
have existed for several years, the older apects are now being combined with a method developed in Karl Deisseroth's lab. By inserting a small fiberoptic cable into the brain the light impulses can be controlled as they search for the affected neurons. This procedure allows for smaller and smaller targets of the G-protein on the specific neuron.The current procedures were developed by under the direction of Karl Deisseroth, MD, PhD at Stanford University. The project required the work of bioengineering and medical neuroscience and neurology students and faculty as they explored target after target to finally find that stimulation of the axons that connect the subthalmic nucleus are actually in areas closer to the brain's surface. While treatments would be still invasive, they would be less invasive thanks to better targeting at the G protein coupled receptors at the cell surface.
 At Stanford University scientists were able to incorporate the technique in model mouse brains to produce activity in a real-time frame using both blue light to signal activity and yellow light to stop. The cells returned to their normal status unchanged at completion.
At Stanford University scientists were able to incorporate the technique in model mouse brains to produce activity in a real-time frame using both blue light to signal activity and yellow light to stop. The cells returned to their normal status unchanged at completion.An interesting thing about neurons is that they communicate in a manner similar to binary code. Sometimes on sometimes off similar to the 0s and 1s of binary code. By being able to communicate in their on-off patterns, learning the neuron language might enable direct actual neural instruction through the flashing of the blue and yellow lights. In another metaphor, Optogenics appears to be the cell tower, now what is needed is a phonebook.
Optogenics holds hope for spinal cord injuries, restoring function to paralyzed limbs, allowing for new therapies, closely targeted pharmaecuticals and possibly become a neuronal therapy in itself.
Optogenics: A process by which brain cells can be activated by specific light
Channel Rhodopsins (ChR): light-activated ion channels appear to be coupled with the photoreceptor so that they do not require chemical signalling but instead are triggered by light.
Channel Rhodopsin (ChR2): algae-derived gene protein which makes neurons more active upon blue light exposure. Currently vector-introduced to the desired neurons. This is the "emit a signal" protein
Halo-rhodopsin (NpHR): from a microbe which can make neurons less active. The instruction here is to "stop emitting." They respond to yellow light.
G protein coupled receptors (GPCRs): signalling proteins found on the surface of nearly all cells.
Reading List:
http://storybank.stanford.edu/stories/controlling-brain-with-optogenics
http://www.newscientist.com/article/dn16807
http://www.freepatentsonline.com/7488583.html
http://pubs.acs.org/cen/science/86/8612sci1.html
http://www2.hu-berlin.de/biologie/expbp/Homepage-new_10408.pdf
http://web.mit.edu/newsoffice/2007/brain-block.html
http://med.stanford.edu/news_releases/2009/march/deisseroth.html
http://storybank.stanford.edu/stories/neural-traffic-light-a-go-better-brain-research
http://www.medicalnewstoday.com/articles/143132.php
In 2014 a small clinical trial for use of CBD oil for seizure disorders was published. It is referenced because of the explanation of the G-protein.
You can now find numerous optogenics studies.
You might also enjoy this article about Karl Deisseroth
2015 Optogenics study: Illuminating Parkinson's Therapy with Optogenics
Wednesday, March 25, 2009
DBS Surgery Basics for Parkinson's Disease
Treatments for PD: Deep Brain Stimulation
We already know that not all PD patients are eligible for Deep Brain Stimulation and that it appears to be effective for some but not all of the people who do receive the treatment. DBS is used in some advanced stages of PD that do not respond well to meds in order to reduce tremors and involuntary movement. It is used in younger and older patients alike. According to CNN, more that 35,000 people have undergone the procedure worldwide. According to one study when successful, DBS a 71% showed an increase in "on" time to about 4.6 hours. In that study about 40% of the patients demonstrated some adverse affects.
Deep brain stimulation (DBS) is a surgical procedure which consists of implanting high frequency electrodes in the subthalmic nucleus (movement center) in order to stimulate neurons to produce brain-derived neurotrophic factor (BDNF) through an implanted pacemaker-like device. Essentially the surgery when successful interrupts the faulty signals of dopamine cell loss. It targets the subthalmic nucleus, thalmus or globus pallidus as predetermined through an MRI or CT. The result is that many Parkinson's patients who receive the treatment find that they require less medication for the PD symptoms they have. The PD treatment is given unilaterally to many patients, bilaterally to others. Some opt for one side only to determine who it will work for them.
The complicated procedure is not without its negative side effects in some cases. There have been neuro-cognitive changes even when there is improvement in motor function. Depression, falls, gait disturbance, motor dysfunction, dystonia, balance and cardiac issues are also side effects in some patients. Sometimes there are infections at the pacemaker site which is usually in the chest. These symptoms may depend upon where the electrodes are placed. If Optogenics is developed to the point of state of the art for PD and use in DBS, we will certainly see far more precision in the placement of the electrodes.
The procedure itself occurs under local anesthetic so that the patient can be awake. The patient's head is immobilized in a frame and an MRI is done to pinpoint where the electrode is to be implanted. Two incisions are made in the skull and the microelectrode is passed into the brain. Current is passed through the electrode and increased while the patients responds to questions and performs certain movement tasks. After trial and error, the correct location is determined and the permanent electrode is placed and secured. The hospital stay is usually a few days.
After the swelling has subsided usually about a week later, the neurostimulator wires are connected to the electrodes. The pacemaker is placed usually in the chest. It may be another two to four weeks before it is turned on. In theory the patients can control the current flow through the pacemaker which is usually implanted in the patient's chest. In actuality the patient meets with the neurologist several times for stimulator adjustment.
The stimulation can be adjusted or turned off unlike the thalamotomy which Michael J Fox underwent seven years after his diagnosis, DBS is reversible in that it can be turned off or adjusted as in cases where tremors recur. When sucessful, the results of DBS can be a radical and remarkable change.
DBS is being used as an alternative therapy to thalamotony and pallidotomy which are permanent irreversible surgical procedures, It is used for control of PD tremor and control of essential tremor. It is being investigated for primary dystonia (involuntary muscle contractions) as well as for intractable epilepsy, cluster headaches which are usually vascular and associated with high blood pressure, chronic intractable pain, morbid obesity and obsessive-compulsive behavior (OCD)
One thng that is important to remember if you are considering Deep Brain Surgery is the Neurosurgical Team that will be performing the surgery. Don't be afraid to ask those questions about their experience and track record. Patients need to be proactive about their treatments.
DBS is not an inexpensive surgery. Costs can vary from $50,000 to $120,000 although in many cases are covered by Medicare and private insurance. Nonetheless, the co-pay can be very high.
In most clinical trials, patients with atypical symptoms, surgical contraindications such as MRIs or past PD surgery are excluded. Most studies will take both genders up to 75 or 80 years of age. What is necessary is that patients must fully disclose their medical history which includes psychiatric history; a desire for the surgery without full disclosure can lead to unexpected side effects.
So who does DBS work for or rather why does it work? How are the cells calmed or stimulated by the electrical shocks they receive? That still isn't clear but researchers in Scotland are exploring the idea that by stimulating other areas perhaps they can affect postural symptoms and gait issues also. One thing that is known is that when successful, DBS can improve the quality of life for the recipient.
Addendum:
On April of 2009, 50 DBS experts assembled to share experiences with Deep Brain Surgery procedures. They reached a consensus, per a recent news release issued by the UCLA Los Angeles Newsroom on October 10, 2010.
The findings include the best candidates for DBS; the importance of having an experienced team with an expertise in stereotactic neurosurgery performing the surgery. For some patients, DBS can be used for patients who have had PD surgeries. It is important to remember that certain treatments of the subthalmic nuclei can increase depression. And a reminder that surgery has complications with infection ranking highest.
You can read the full news release at the UCLA website.
References:
The first link is for DBS clinical trials - both closed and recruiting.
VIDEOS about DBS
You can watch video clips for PPN, dystonia and tremor.
And have your choice of many clips at YouTube.
If you live in Norway, there is a DBS clinical trial currently recruiting:
Clinical trial BCT00855621
Contact: Dr Mathias Toft 4799514189
Open to: 18-75 years
Gender: both
To study motor function, quality of life and cognitive function
Who is a good candidate for Deep Brain Stimulation
The medical history of DBS
Coming next:
Spinal Cord Stimulation
Optogenics
Magnetic Stimulation
We already know that not all PD patients are eligible for Deep Brain Stimulation and that it appears to be effective for some but not all of the people who do receive the treatment. DBS is used in some advanced stages of PD that do not respond well to meds in order to reduce tremors and involuntary movement. It is used in younger and older patients alike. According to CNN, more that 35,000 people have undergone the procedure worldwide. According to one study when successful, DBS a 71% showed an increase in "on" time to about 4.6 hours. In that study about 40% of the patients demonstrated some adverse affects.
Deep brain stimulation (DBS) is a surgical procedure which consists of implanting high frequency electrodes in the subthalmic nucleus (movement center) in order to stimulate neurons to produce brain-derived neurotrophic factor (BDNF) through an implanted pacemaker-like device. Essentially the surgery when successful interrupts the faulty signals of dopamine cell loss. It targets the subthalmic nucleus, thalmus or globus pallidus as predetermined through an MRI or CT. The result is that many Parkinson's patients who receive the treatment find that they require less medication for the PD symptoms they have. The PD treatment is given unilaterally to many patients, bilaterally to others. Some opt for one side only to determine who it will work for them.
The complicated procedure is not without its negative side effects in some cases. There have been neuro-cognitive changes even when there is improvement in motor function. Depression, falls, gait disturbance, motor dysfunction, dystonia, balance and cardiac issues are also side effects in some patients. Sometimes there are infections at the pacemaker site which is usually in the chest. These symptoms may depend upon where the electrodes are placed. If Optogenics is developed to the point of state of the art for PD and use in DBS, we will certainly see far more precision in the placement of the electrodes.
The procedure itself occurs under local anesthetic so that the patient can be awake. The patient's head is immobilized in a frame and an MRI is done to pinpoint where the electrode is to be implanted. Two incisions are made in the skull and the microelectrode is passed into the brain. Current is passed through the electrode and increased while the patients responds to questions and performs certain movement tasks. After trial and error, the correct location is determined and the permanent electrode is placed and secured. The hospital stay is usually a few days.
After the swelling has subsided usually about a week later, the neurostimulator wires are connected to the electrodes. The pacemaker is placed usually in the chest. It may be another two to four weeks before it is turned on. In theory the patients can control the current flow through the pacemaker which is usually implanted in the patient's chest. In actuality the patient meets with the neurologist several times for stimulator adjustment.
The stimulation can be adjusted or turned off unlike the thalamotomy which Michael J Fox underwent seven years after his diagnosis, DBS is reversible in that it can be turned off or adjusted as in cases where tremors recur. When sucessful, the results of DBS can be a radical and remarkable change.
DBS is being used as an alternative therapy to thalamotony and pallidotomy which are permanent irreversible surgical procedures, It is used for control of PD tremor and control of essential tremor. It is being investigated for primary dystonia (involuntary muscle contractions) as well as for intractable epilepsy, cluster headaches which are usually vascular and associated with high blood pressure, chronic intractable pain, morbid obesity and obsessive-compulsive behavior (OCD)
One thng that is important to remember if you are considering Deep Brain Surgery is the Neurosurgical Team that will be performing the surgery. Don't be afraid to ask those questions about their experience and track record. Patients need to be proactive about their treatments.
DBS is not an inexpensive surgery. Costs can vary from $50,000 to $120,000 although in many cases are covered by Medicare and private insurance. Nonetheless, the co-pay can be very high.
In most clinical trials, patients with atypical symptoms, surgical contraindications such as MRIs or past PD surgery are excluded. Most studies will take both genders up to 75 or 80 years of age. What is necessary is that patients must fully disclose their medical history which includes psychiatric history; a desire for the surgery without full disclosure can lead to unexpected side effects.
So who does DBS work for or rather why does it work? How are the cells calmed or stimulated by the electrical shocks they receive? That still isn't clear but researchers in Scotland are exploring the idea that by stimulating other areas perhaps they can affect postural symptoms and gait issues also. One thing that is known is that when successful, DBS can improve the quality of life for the recipient.
Addendum:
On April of 2009, 50 DBS experts assembled to share experiences with Deep Brain Surgery procedures. They reached a consensus, per a recent news release issued by the UCLA Los Angeles Newsroom on October 10, 2010.
The findings include the best candidates for DBS; the importance of having an experienced team with an expertise in stereotactic neurosurgery performing the surgery. For some patients, DBS can be used for patients who have had PD surgeries. It is important to remember that certain treatments of the subthalmic nuclei can increase depression. And a reminder that surgery has complications with infection ranking highest.
You can read the full news release at the UCLA website.
References:
The first link is for DBS clinical trials - both closed and recruiting.
VIDEOS about DBS
You can watch video clips for PPN, dystonia and tremor.
And have your choice of many clips at YouTube.
If you live in Norway, there is a DBS clinical trial currently recruiting:
Clinical trial BCT00855621
Contact: Dr Mathias Toft 4799514189
Open to: 18-75 years
Gender: both
To study motor function, quality of life and cognitive function
Who is a good candidate for Deep Brain Stimulation
The medical history of DBS
Coming next:
Spinal Cord Stimulation
Optogenics
Magnetic Stimulation
Saturday, March 21, 2009
The Nose Knows
Loss of Sense of Smell in Parkinson's Disease
 I noticed I was losing my sense of smell before I realized I had the symptoms of Parkinson's disease. For many PD patients that loss is their first inkling that something is wrong. Over 20 million people suffer from loss of sense of smell in the US. It can be caused by allergies, viral infections or chronic neurological conditions such as Multiple Sclerosis, Alzheimer's or Parkinson's disease.
I noticed I was losing my sense of smell before I realized I had the symptoms of Parkinson's disease. For many PD patients that loss is their first inkling that something is wrong. Over 20 million people suffer from loss of sense of smell in the US. It can be caused by allergies, viral infections or chronic neurological conditions such as Multiple Sclerosis, Alzheimer's or Parkinson's disease.
The sense of smell is part of our chemical sensing system. Sensory cells in our noses, mouths and throats help us interpret smells and the favors of food and drink. Microscopic molecules released by the plants and foods around us stimulate these sensor cells to signal the brain which is where scents are identified.
Sensory cells in our noses, mouths and throats help us interpret smells and the favors of food and drink. Microscopic molecules released by the plants and foods around us stimulate these sensor cells to signal the brain which is where scents are identified.
The loss of the ability to smell can be dangerous. We are warned of a fire by the smell of smoke. Smell is often the first warning of a natural gas or propane leak. More important is that the loss of sense of smell is a warning of impending health problems: obesity, diabetes, hypertension, malnutrition, Parkinson's, MS, Alzheimer's can all be signaled by the loss or partial loss of the sense of smell.
It's been 10 or 15 years since I have been able to sense smells normally. I seem to be lucky that I can still taste foods with my mouth and throat aided by freshly ground red or black pepper or curry powder. Mostly I try not to agonize over my lost senses. I think the best answer is to try developing a love for remaining senses.
Some people can be treated successfully. A drug interaction could be the cause of olfactory loss might be correctable. Changing a medicine might work or for some a spontaneous recovery might be caused by the regeneration of the olfactory neurons. I tried zinc ascorbate last month and it did restore some slight ability to taste and smell but my wife took it away from me after 30 days telling me that I would have to wait a month or so before using it again for 30 days.
Some people have found that by taking theophylline, a broncodilator to relax smooth muscle contraction, they have regained their sense of smell. This is not recommendation, it is an observation indicating that there will be safer pathways developed.
contraction, they have regained their sense of smell. This is not recommendation, it is an observation indicating that there will be safer pathways developed.
Olfactory research is going on at universities and medical centers across the US. Some research is showing scientists how the parts of the olfactory system which sense and identify smells interact with other physical and neurological parts of the olfactory system.
Perhaps, as the result of treatments developed in the next few years, I will be able to sit with my wife and savour a meal that I will remember the rest of my life, like the one in Montreal 40 years ago that I'm remembering now.
Addendum 2010
Refer a friend or relative to the PARS - Parkinson Associated Risk Study.
Although the study initially wanted people with first-degree relatives, they soon found that it didn't make a difference if the person was a relative of a PWP or not. While they prefer people over 60 years of age, people with a family member with PD may be eligible if under 60.
The goal is to study early warning signs. We all know that early diagnosis means that treatment can be initiated sooner. Now that we know there is more than one treatment or therapy which might slow progression, early diagnosis becomes more imperative.
Addendum 11/2015
New Parkinson's disease diagnostics are being developed by a 4 continent task force, the International Parkinson and Movement Disorder Society (MDS) task force.
According to a Foxfeed blog entry posted by Maggie McGuire Kuhl on 11/23/2015, Dr Robert B Postuma of Montreal General Hospital had this to say about using loss of sense of smell in both diagnosis and in differential diagnosis.
It’s a supportive criterion because we know that 80 percent of Parkinson’s patients have lost their sense of smell. And up to 80 percent of people who have alternate causes (PSP, MSA, essential or dystonic tremor) have normal smell.
 I noticed I was losing my sense of smell before I realized I had the symptoms of Parkinson's disease. For many PD patients that loss is their first inkling that something is wrong. Over 20 million people suffer from loss of sense of smell in the US. It can be caused by allergies, viral infections or chronic neurological conditions such as Multiple Sclerosis, Alzheimer's or Parkinson's disease.
I noticed I was losing my sense of smell before I realized I had the symptoms of Parkinson's disease. For many PD patients that loss is their first inkling that something is wrong. Over 20 million people suffer from loss of sense of smell in the US. It can be caused by allergies, viral infections or chronic neurological conditions such as Multiple Sclerosis, Alzheimer's or Parkinson's disease. The sense of smell is part of our chemical sensing system.
 Sensory cells in our noses, mouths and throats help us interpret smells and the favors of food and drink. Microscopic molecules released by the plants and foods around us stimulate these sensor cells to signal the brain which is where scents are identified.
Sensory cells in our noses, mouths and throats help us interpret smells and the favors of food and drink. Microscopic molecules released by the plants and foods around us stimulate these sensor cells to signal the brain which is where scents are identified. The loss of the ability to smell can be dangerous. We are warned of a fire by the smell of smoke. Smell is often the first warning of a natural gas or propane leak. More important is that the loss of sense of smell is a warning of impending health problems: obesity, diabetes, hypertension, malnutrition, Parkinson's, MS, Alzheimer's can all be signaled by the loss or partial loss of the sense of smell.
Loss of the sense of smell as well as the sense of taste is a PD symptom that can also cause depression. As the pleasure derived from tasting and smelling wane, the world can seem a bit less interesting. Without even realizing what it is that we miss at first, we know that a source of pleasure has disappeared from our lives.
It's been 10 or 15 years since I have been able to sense smells normally. I seem to be lucky that I can still taste foods with my mouth and throat aided by freshly ground red or black pepper or curry powder. Mostly I try not to agonize over my lost senses. I think the best answer is to try developing a love for remaining senses.
Some people can be treated successfully. A drug interaction could be the cause of olfactory loss might be correctable. Changing a medicine might work or for some a spontaneous recovery might be caused by the regeneration of the olfactory neurons. I tried zinc ascorbate last month and it did restore some slight ability to taste and smell but my wife took it away from me after 30 days telling me that I would have to wait a month or so before using it again for 30 days.
Some people have found that by taking theophylline, a broncodilator to relax smooth muscle
 contraction, they have regained their sense of smell. This is not recommendation, it is an observation indicating that there will be safer pathways developed.
contraction, they have regained their sense of smell. This is not recommendation, it is an observation indicating that there will be safer pathways developed.Olfactory research is going on at universities and medical centers across the US. Some research is showing scientists how the parts of the olfactory system which sense and identify smells interact with other physical and neurological parts of the olfactory system.
Perhaps, as the result of treatments developed in the next few years, I will be able to sit with my wife and savour a meal that I will remember the rest of my life, like the one in Montreal 40 years ago that I'm remembering now.
Addendum 2010
Refer a friend or relative to the PARS - Parkinson Associated Risk Study.
Although the study initially wanted people with first-degree relatives, they soon found that it didn't make a difference if the person was a relative of a PWP or not. While they prefer people over 60 years of age, people with a family member with PD may be eligible if under 60.
The goal is to study early warning signs. We all know that early diagnosis means that treatment can be initiated sooner. Now that we know there is more than one treatment or therapy which might slow progression, early diagnosis becomes more imperative.
Addendum 11/2015
New Parkinson's disease diagnostics are being developed by a 4 continent task force, the International Parkinson and Movement Disorder Society (MDS) task force.
According to a Foxfeed blog entry posted by Maggie McGuire Kuhl on 11/23/2015, Dr Robert B Postuma of Montreal General Hospital had this to say about using loss of sense of smell in both diagnosis and in differential diagnosis.
It’s a supportive criterion because we know that 80 percent of Parkinson’s patients have lost their sense of smell. And up to 80 percent of people who have alternate causes (PSP, MSA, essential or dystonic tremor) have normal smell.
Friday, March 20, 2009
Brain Stimulation Breakthrough for Parkinson's Disease
Possible PD treatment without risky surgery
 Today I've been reading a fascinating article in the New York Times about a recent new approach to treating Parkinson's disease. It describes spinal cord stimulation in dopamine-deprived rats where a mild electrical current flows up the rodent's spinal cord and into the brain. As long as that current is maintained the rodents regain their ability to move normally.
Today I've been reading a fascinating article in the New York Times about a recent new approach to treating Parkinson's disease. It describes spinal cord stimulation in dopamine-deprived rats where a mild electrical current flows up the rodent's spinal cord and into the brain. As long as that current is maintained the rodents regain their ability to move normally.
This procedure in being tested in monkeys now because humans and monkeys are the only two species which get PD naturally. If it is proven to be safe and efficient, spinal cord stimulation will be a potential alternative to DBS since it requires no risky invasive surgery to plant electrodes deep in the brain. It may be effective for some of the 70% of severely impaired PDers who do not qualify for deep brain stimulation.
This could represent a major paradigm shift in available treatments. It is not without drawbacks-tradeoffs, however since one side effect is reported to be a never-ending mini-vibration described by Dr Ali Rezai, director of the Cleveland Clinic Center for Neurological Restoration as "pins and needles."
Read more:
http://www.nytimes.com/2009/03/20/health/20spinal.html?_r=1&ref=health
 Today I've been reading a fascinating article in the New York Times about a recent new approach to treating Parkinson's disease. It describes spinal cord stimulation in dopamine-deprived rats where a mild electrical current flows up the rodent's spinal cord and into the brain. As long as that current is maintained the rodents regain their ability to move normally.
Today I've been reading a fascinating article in the New York Times about a recent new approach to treating Parkinson's disease. It describes spinal cord stimulation in dopamine-deprived rats where a mild electrical current flows up the rodent's spinal cord and into the brain. As long as that current is maintained the rodents regain their ability to move normally.This procedure in being tested in monkeys now because humans and monkeys are the only two species which get PD naturally. If it is proven to be safe and efficient, spinal cord stimulation will be a potential alternative to DBS since it requires no risky invasive surgery to plant electrodes deep in the brain. It may be effective for some of the 70% of severely impaired PDers who do not qualify for deep brain stimulation.
This could represent a major paradigm shift in available treatments. It is not without drawbacks-tradeoffs, however since one side effect is reported to be a never-ending mini-vibration described by Dr Ali Rezai, director of the Cleveland Clinic Center for Neurological Restoration as "pins and needles."
Read more:
http://www.nytimes.com/2009/03/20/health/20spinal.html?_r=1&ref=health
Thursday, March 19, 2009
Parkinson's Disease Research - Part II
Reprogrammed Skin Cells for Parkinson's
There are other methods for developing effective treatments and possibly cures for diseases through the adaptation of non-embryonic stem cells which are induced to have the pluripotent capabilities. There appears to be potential if these cells can live up to their promise.
Induced pluripotent cells
Non-embryonic stem cells induced/stimulated to
become pluripotent (iPS)
Embryonic stem cells
Already pluripotent (ESC) capable of being any cell
hESC
Human embryonic stem cells
hiPSC
Human induced pluripotent cells
Pluripotent
having the capability to be any cell
Gene expression
a measure of which genes the cell uses and how much of the
cell uses those genes
Genetic recombination
a strand of genetic material (DNA or sometimes RNA)
is broken and joined to a different DNA molecule
Botanists have been grafting for centuries but this is nano
micro-scale and complicated
Cre recombinase
Enzyme which catalyzes genetic recombination
Transgene
Genetic material transferredfrom one organism to another;
any DNA sequence introduced into an organism.
Factor-free
without being introduced via a virus factor
As you already know, researchers in Cambridge MA have been able to use skin cells which were induced into pluripotency to become dopamine-producing neuron cells. Unlike previous research, these iPS did not insert cancer producing genes into the DNA because that reprogramming was removed allowing the cells to maintain an ESC-like status.
The problem in the past has been that the reprogrammed cells had the potential to cause cancer, creating an out of the frying pan and into the fire situation. In the new process: the skin cells of a Parkinson's patient are reprogrammed to be iPS cells. And then reprogrammed again so that the potentially cancer-causing program was removed. At this point the human induced pluripotent cells (hiPS) are very similar to human embryonic stem cells (hESC)
In the past researchers were not sure that removing the reprogramming from these human cells would allow the cell to maintain a stable iPS state so that it could multiply. Now they are. This step opens the door...
Links:
http://www.cell.com/abstract/S0092-8674(09)00151-2
http://esciencenews.com/articles/2009/03/05/breakthrough.produces.parkinsons.patient.specific.stem.cells.free.harmful.reprogramming.genes
The Scientists:
Whitehead Institute for Biomedical Research, Cambridge, Mass: Frank Soldner, Dirk Hockemeyer, Caroline Beard, George W Bell, Elizabeth G Cook, Qing Gao, Miasam Mitalippova, Rudolph Jaenisch
Dept of Biology MIT, Cambridge, Mass: Rudolph Jaenisch
Udall Parkinson Disease Research Center of Excellence, Center for Neuroredegeneration Research, McLean Hospital/Harvard Medical School, Cambridge, Mass: Gunnar Hargus, Alexandra Blak, Oliver Cooper, Ole Isacson
There are other methods for developing effective treatments and possibly cures for diseases through the adaptation of non-embryonic stem cells which are induced to have the pluripotent capabilities. There appears to be potential if these cells can live up to their promise.
Induced pluripotent cells
Non-embryonic stem cells induced/stimulated to
become pluripotent (iPS)
Embryonic stem cells
Already pluripotent (ESC) capable of being any cell
hESC
Human embryonic stem cells
hiPSC
Human induced pluripotent cells
Pluripotent
having the capability to be any cell
Gene expression
a measure of which genes the cell uses and how much of the
cell uses those genes
Genetic recombination
a strand of genetic material (DNA or sometimes RNA)
is broken and joined to a different DNA molecule
Botanists have been grafting for centuries but this is nano
micro-scale and complicated
Cre recombinase
Enzyme which catalyzes genetic recombination
Transgene
Genetic material transferredfrom one organism to another;
any DNA sequence introduced into an organism.
Factor-free
without being introduced via a virus factor
As you already know, researchers in Cambridge MA have been able to use skin cells which were induced into pluripotency to become dopamine-producing neuron cells. Unlike previous research, these iPS did not insert cancer producing genes into the DNA because that reprogramming was removed allowing the cells to maintain an ESC-like status.
The problem in the past has been that the reprogrammed cells had the potential to cause cancer, creating an out of the frying pan and into the fire situation. In the new process: the skin cells of a Parkinson's patient are reprogrammed to be iPS cells. And then reprogrammed again so that the potentially cancer-causing program was removed. At this point the human induced pluripotent cells (hiPS) are very similar to human embryonic stem cells (hESC)
In the past researchers were not sure that removing the reprogramming from these human cells would allow the cell to maintain a stable iPS state so that it could multiply. Now they are. This step opens the door...
Links:
http://www.cell.com/abstract/S0092-8674(09)00151-2
http://esciencenews.com/articles/2009/03/05/breakthrough.produces.parkinsons.patient.specific.stem.cells.free.harmful.reprogramming.genes
The Scientists:
Whitehead Institute for Biomedical Research, Cambridge, Mass: Frank Soldner, Dirk Hockemeyer, Caroline Beard, George W Bell, Elizabeth G Cook, Qing Gao, Miasam Mitalippova, Rudolph Jaenisch
Dept of Biology MIT, Cambridge, Mass: Rudolph Jaenisch
Udall Parkinson Disease Research Center of Excellence, Center for Neuroredegeneration Research, McLean Hospital/Harvard Medical School, Cambridge, Mass: Gunnar Hargus, Alexandra Blak, Oliver Cooper, Ole Isacson
Wednesday, March 18, 2009
Parkinson's Disease Research Basics - Part I
Information about stem cells and stem cell research for PD
Let's do a quick summary of stem cells. They are the cells which can renew themselves through the process of mitosis. Once the nuclei separate the chromosomes to replicate itself, the cell can then split to form two identical cells with the second cell carrying all of the genetic information as the first.
In the body there are two types of stem cells, adult and embryonic. The adult stem cell is the repairman/woman, some being very versatile themselves. The embryonic stem cell (ESC) can differentiate itself into all of the specialized tissues...functions. It is for this reason that it is known as a pluripotent cell. (Preceding the pluripotent cell is the totipotent cell but that is another story.) The stem cell creates the existence of all three germ layers which form the body.
A stem cell line is a family of cells from one parent group. They require the correct signaling in order to differentiate into the cells required. This is where the research picks up.
The first stem cell lines were created in 1988 at the University of Wisconsin-Madison. Dr James A Thompson's directed the group which isolated the first human embryonic stem cells, those undifferentiated cells which can multiply in the body. Currently at UW-M they are working to understand the mechanism by which embryonic stem cells can form any body cell (pluripotency), how that cell chooses between self-renewal and differentiation, and how the differentiated cell can be reprogrammed for pluripotency.
If you look up the National Stem Cell Registry online you will see the NIH website. One of the topics which gave us a big smile was the link to an archive entitled, Registry Information Under the Former Presidential Policy.
Here is the National Institute of Health stem cell site. If you haven't been there yet, check it out some time.
http://stemcells.nih.gov/
President Obama's Executive Order was not a complete green light for embryonic stem cell research. It did lift the ban on a few lines that were in existence as of 8/09/01 and has been interpreted to mean that new stem cell lines may be developed. The NIH has the responsibility to determine the guidlines for what scientists can do with federal monies.
NIH will receive $10.4 billion stimulus money from the American Recovery and Reinvestment Act. $3 billion will go to the National Science Foundation which already has $2 billion in approved but unfunded grants.
Something we were pleased to see at the NIH site were the links to what is happening in Congress. These are earlier pieces of legislation which are moving through the legislative process. The full text of each is available at the Library of Congress website links. You can link to the site and read the text of each pending Act.
111th Congress, House Bills
H.R. 110—Human Cloning Prohibition Act of 2009
H.R. 872—Stem Cell Research Improvement Act of 2009 H.R. 873—Stem Cell Research Enhancement Act of 2009
H.R. 873—Stem Cell Research Enhancement Act of 2009
H.R. 877—Patients First Act of 2009
111th Congress, Senate Bill
S. 99—Ethical Stem Cell Research Tax Credit Act of 2009
While these things are going on in D.C. several states have already passed legislation encouraging and sometimes funding stem cell research. Maryland, New Jersey, New York, Connecticut, Massachusetts, Illinois, Iowa and California passed programs authorizing research spending after the 2001 federal ban. These programs are costly and some states have had to limit funding in the current economy so it is hoped that donations will not stop although many private philanthropies have been devastated recently.
On November 4, 2008 Michigan saw the passage of a state constitutional amendment which would permit researchers to create new stem cell lines by using surplus embryos from fertility clinics.
In contrast Oklahoma and Georgia have taken an opposite position and are presenting legislative action to restore the Bush status quo. In Georgia the senate has already passed legislation to prevent using cloning to create human embryos. The bill does allow induced pluripotent stem cells (iPS) which we will discuss tomorrow.
Arizona, Louisiana, Mississippi and Texas already have laws on the books concerning use of state funds for research which would destroy a human embryo, would manipulate stem cells for treatment or potential cures or conduct research using the in vitro clinic (IVF) discards.
Most stem cells used in research have come from unused embryos of fertility clinics. They were at a "use 'em or lose 'em" condition. Since they were not going to be used in an attempt to create new humans, they would have been discarded if there had not been another use for research to develop a way to save existing human lives. There is a fear that in the future other sources which do not police themselves will be used.
Meanwhile there is much work to be done to develop effective, safe treatments.
A few places which have received federal grants for stem cell research recently or are sponsoring stem cell research:
University of Buffalo just received $4.9 million.
In Michigan on March 9th the University of Michigan announced a $5 million initiative with the Alfred A Taubman Medical Research Institute Consortium for Stem Cell Research. The consortium could also collaborate with with the University Research Corridor partners: Michigan State University, Wayne State University, Oakland University, University of Michigan at Dearborn as well as Case Western Reserve University in Cleveland, Ohio. They will be looking to create new stem cell lines from IVF clinics using the International Society for Research guidelines (see: link in FAQs below.)
California's Stem Cell Agency announced $17.5 million in grants for embryonic stem cell technology: training students in lab work, research techniques and ethics in a program which can lead to a masters degree.
Research being sponsored by:
http://www.parkinsons.org.uk/research/current-research/ongoing-stem-cell-research.aspx
http://www.michaeljfox.org/research_MJFFfundingPortfolio_searchableAwardedGrants_2.cfm?Search=Yes&ProgramID=3&Keyword1=42&Keyword2=&Country=&State=&Last_Name=&Institution=&Grant_Funded_Year=&search.x=28&search.y=9
FAQ links:
http://stemcells.nih.gov/info/basics/
http://www.isscr.org/science/faq.htm
http://stemcells.nih.gov/StemCells/Templates/StemCellContentPage.aspx?NRMODE=Published&NRNODEGUID=%7bA604DCCE-2E5F-4395-8954-FCE1C05BECED%7d&NRORIGINALURL=%2finfo%2ffaqs%2easp&NRCACHEHINT=NoModifyGuest#excited
http://www.aaas.org/spp/sfrl/projects/stem/index.shtml
Information about embryonic stem cell research for other conditions
http://www.geron.com/grnopc1clearance/
The National Stem Cell Bank: http://www.nationalstemcellbank.org/
Let's do a quick summary of stem cells. They are the cells which can renew themselves through the process of mitosis. Once the nuclei separate the chromosomes to replicate itself, the cell can then split to form two identical cells with the second cell carrying all of the genetic information as the first.
In the body there are two types of stem cells, adult and embryonic. The adult stem cell is the repairman/woman, some being very versatile themselves. The embryonic stem cell (ESC) can differentiate itself into all of the specialized tissues...functions. It is for this reason that it is known as a pluripotent cell. (Preceding the pluripotent cell is the totipotent cell but that is another story.) The stem cell creates the existence of all three germ layers which form the body.
A stem cell line is a family of cells from one parent group. They require the correct signaling in order to differentiate into the cells required. This is where the research picks up.
The first stem cell lines were created in 1988 at the University of Wisconsin-Madison. Dr James A Thompson's directed the group which isolated the first human embryonic stem cells, those undifferentiated cells which can multiply in the body. Currently at UW-M they are working to understand the mechanism by which embryonic stem cells can form any body cell (pluripotency), how that cell chooses between self-renewal and differentiation, and how the differentiated cell can be reprogrammed for pluripotency.
If you look up the National Stem Cell Registry online you will see the NIH website. One of the topics which gave us a big smile was the link to an archive entitled, Registry Information Under the Former Presidential Policy.
Here is the National Institute of Health stem cell site. If you haven't been there yet, check it out some time.
http://stemcells.nih.gov/
President Obama's Executive Order was not a complete green light for embryonic stem cell research. It did lift the ban on a few lines that were in existence as of 8/09/01 and has been interpreted to mean that new stem cell lines may be developed. The NIH has the responsibility to determine the guidlines for what scientists can do with federal monies.
NIH will receive $10.4 billion stimulus money from the American Recovery and Reinvestment Act. $3 billion will go to the National Science Foundation which already has $2 billion in approved but unfunded grants.
Something we were pleased to see at the NIH site were the links to what is happening in Congress. These are earlier pieces of legislation which are moving through the legislative process. The full text of each is available at the Library of Congress website links. You can link to the site and read the text of each pending Act.
111th Congress, House Bills
H.R. 110—Human Cloning Prohibition Act of 2009
H.R. 872—Stem Cell Research Improvement Act of 2009 H.R. 873—Stem Cell Research Enhancement Act of 2009
H.R. 873—Stem Cell Research Enhancement Act of 2009
H.R. 877—Patients First Act of 2009
111th Congress, Senate Bill
S. 99—Ethical Stem Cell Research Tax Credit Act of 2009
While these things are going on in D.C. several states have already passed legislation encouraging and sometimes funding stem cell research. Maryland, New Jersey, New York, Connecticut, Massachusetts, Illinois, Iowa and California passed programs authorizing research spending after the 2001 federal ban. These programs are costly and some states have had to limit funding in the current economy so it is hoped that donations will not stop although many private philanthropies have been devastated recently.
On November 4, 2008 Michigan saw the passage of a state constitutional amendment which would permit researchers to create new stem cell lines by using surplus embryos from fertility clinics.
In contrast Oklahoma and Georgia have taken an opposite position and are presenting legislative action to restore the Bush status quo. In Georgia the senate has already passed legislation to prevent using cloning to create human embryos. The bill does allow induced pluripotent stem cells (iPS) which we will discuss tomorrow.
Arizona, Louisiana, Mississippi and Texas already have laws on the books concerning use of state funds for research which would destroy a human embryo, would manipulate stem cells for treatment or potential cures or conduct research using the in vitro clinic (IVF) discards.
Most stem cells used in research have come from unused embryos of fertility clinics. They were at a "use 'em or lose 'em" condition. Since they were not going to be used in an attempt to create new humans, they would have been discarded if there had not been another use for research to develop a way to save existing human lives. There is a fear that in the future other sources which do not police themselves will be used.
Meanwhile there is much work to be done to develop effective, safe treatments.
A few places which have received federal grants for stem cell research recently or are sponsoring stem cell research:
University of Buffalo just received $4.9 million.
In Michigan on March 9th the University of Michigan announced a $5 million initiative with the Alfred A Taubman Medical Research Institute Consortium for Stem Cell Research. The consortium could also collaborate with with the University Research Corridor partners: Michigan State University, Wayne State University, Oakland University, University of Michigan at Dearborn as well as Case Western Reserve University in Cleveland, Ohio. They will be looking to create new stem cell lines from IVF clinics using the International Society for Research guidelines (see: link in FAQs below.)
California's Stem Cell Agency announced $17.5 million in grants for embryonic stem cell technology: training students in lab work, research techniques and ethics in a program which can lead to a masters degree.
Research being sponsored by:
http://www.parkinsons.org.uk/research/current-research/ongoing-stem-cell-research.aspx
http://www.michaeljfox.org/research_MJFFfundingPortfolio_searchableAwardedGrants_2.cfm?Search=Yes&ProgramID=3&Keyword1=42&Keyword2=&Country=&State=&Last_Name=&Institution=&Grant_Funded_Year=&search.x=28&search.y=9
FAQ links:
http://stemcells.nih.gov/info/basics/
http://www.isscr.org/science/faq.htm
http://stemcells.nih.gov/StemCells/Templates/StemCellContentPage.aspx?NRMODE=Published&NRNODEGUID=%7bA604DCCE-2E5F-4395-8954-FCE1C05BECED%7d&NRORIGINALURL=%2finfo%2ffaqs%2easp&NRCACHEHINT=NoModifyGuest#excited
http://www.aaas.org/spp/sfrl/projects/stem/index.shtml
Information about embryonic stem cell research for other conditions
http://www.geron.com/grnopc1clearance/
The National Stem Cell Bank: http://www.nationalstemcellbank.org/
Monday, March 16, 2009
PINK1 Research from London
Why do dopamine cells die?
Here's the problem, we read all of these articles and abstracts and try to make some sense of them but sometimes we find our eyes crossing as the confusion and profusion of terminology mounts. Our goal today is really to talk about the significance of the PINK1 gene and recent research at the Institute of Neurology, London under Dr Andrey G Abramov.
There are several genes which have been identified as being linked to family PD - inherited Parkinson's. Many of these genes "write the code" for the proteins which target the mitochondria. Mutations or misfolding of proteins of PINK1 cause an inherited form of PD identified as an autosomal recessive young onset form of Parkinson's disease. The PINK1 gene is specific to the mitochondria.
Mitochondria = an organelle which is part of a cell - just as an organ is to the body. Some cells have just one while others have thousands.
They power the cell by generating chemical energy in the form of adenosine triphospate (ATP) by converting food molecules into ATP.
And that's not all they do.
They are involved in maintaining proper chemical balances within the cells. They are also involved in signaling, a cellular form of grad school whereby a less specialized cell becomes more specialized. Those cells get their doctorates when they become pluripotent.
Mitochondrial proteins will vary depending upon the tissue type. In PINK1 the protein is serine/theronine kinease.
The mitochondria has two walls, the inner and the outer membrane. The outer membrane is easily permeable to small molecules such as ions and sugars. Large molecules need to have know the password, or to have the correct garage door opener signal if you prefer, in order to be transported through the outer membrane. And then things start to get tricky.
How does this relate to PD? First the bad news. In their role as chemical balancers, mitochondria must maintain the proper calcium level of the cell. Abnormal calcium levels have shown to be toxic to neurons. When the PINK1 gene was studied it was learned that its loss resulted in an abnormal calcium overload within the mitochondria. This calcium overload causes "the production of a dangerous reactive oxygen species that interfered with the ability of the mitochondria to transport sugar for energy production."
A normal PINK1 would be able to handle a calcium overload as that is part of their function. Once they malfunction, they are prone to making the dopamine neurons more vulnerable and may indeed cause their deaths.The good news is that Dr Andrey Abramov and his co-researchers at the Institute Neurology, London, UK have a better understanding of why certain dopamine neurons die.
reference: Cell Press 3/13/09 Molecular Cell
http://www.eurekalert.org/pub_releases/2009-03/cp-pmm030909.php
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2649444
Here's the problem, we read all of these articles and abstracts and try to make some sense of them but sometimes we find our eyes crossing as the confusion and profusion of terminology mounts. Our goal today is really to talk about the significance of the PINK1 gene and recent research at the Institute of Neurology, London under Dr Andrey G Abramov.
There are several genes which have been identified as being linked to family PD - inherited Parkinson's. Many of these genes "write the code" for the proteins which target the mitochondria. Mutations or misfolding of proteins of PINK1 cause an inherited form of PD identified as an autosomal recessive young onset form of Parkinson's disease. The PINK1 gene is specific to the mitochondria.
Mitochondria = an organelle which is part of a cell - just as an organ is to the body. Some cells have just one while others have thousands.
They power the cell by generating chemical energy in the form of adenosine triphospate (ATP) by converting food molecules into ATP.
And that's not all they do.
They are involved in maintaining proper chemical balances within the cells. They are also involved in signaling, a cellular form of grad school whereby a less specialized cell becomes more specialized. Those cells get their doctorates when they become pluripotent.
Mitochondrial proteins will vary depending upon the tissue type. In PINK1 the protein is serine/theronine kinease.
The mitochondria has two walls, the inner and the outer membrane. The outer membrane is easily permeable to small molecules such as ions and sugars. Large molecules need to have know the password, or to have the correct garage door opener signal if you prefer, in order to be transported through the outer membrane. And then things start to get tricky.
How does this relate to PD? First the bad news. In their role as chemical balancers, mitochondria must maintain the proper calcium level of the cell. Abnormal calcium levels have shown to be toxic to neurons. When the PINK1 gene was studied it was learned that its loss resulted in an abnormal calcium overload within the mitochondria. This calcium overload causes "the production of a dangerous reactive oxygen species that interfered with the ability of the mitochondria to transport sugar for energy production."
A normal PINK1 would be able to handle a calcium overload as that is part of their function. Once they malfunction, they are prone to making the dopamine neurons more vulnerable and may indeed cause their deaths.The good news is that Dr Andrey Abramov and his co-researchers at the Institute Neurology, London, UK have a better understanding of why certain dopamine neurons die.
reference: Cell Press 3/13/09 Molecular Cell
http://www.eurekalert.org/pub_releases/2009-03/cp-pmm030909.php
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2649444
Saturday, March 14, 2009
Questions About Parkinson's Disease Part VI - Depression, PD & SAD
Parkinson's Depression and Seasonal Affective Disorder: SAD
 One last area to discuss when speaking about depression is Seasonal Affective Disorder - SAD.
One last area to discuss when speaking about depression is Seasonal Affective Disorder - SAD.
It isn't just the winter blues because you feel cooped in even when you have to go out and about. SAD is more serious than that. It affects patients and caregivers alike. Some people have SAD even in the spring and summer. And treatment can be the same for everyone.
Winter SAD symptoms:
Weight gain
Carb cravings
Oversleeping - waking too early
Indecisiveness
Decreased sex drive
Apathy
Feelings of hopelessness
Anxiety
Suicidal thoughts
Lack of concentration or difficulty concentrating
Difficulty processing information
Summer-Spring SAD symptoms:
Anxiety
Insomnia
Irritability
Agitation
Loss of appetite
Weight loss
Increased sex drive
Yes there is even Reverse SAD which involves manic symptoms which makes sense when you think about it. Symptoms include hypperactivity, increased social activity, extreme enthusiasm, persistent UP mood.
 For roughly 80 percent of SAD sufferers, melatonin levels peak just when it’s time to wake up. For those people, morning light therapy is best. For others, melatonin drops too soon, and they find themselves waking up in the middle of the night. Those patients may find that evening light therapy can work better.
For roughly 80 percent of SAD sufferers, melatonin levels peak just when it’s time to wake up. For those people, morning light therapy is best. For others, melatonin drops too soon, and they find themselves waking up in the middle of the night. Those patients may find that evening light therapy can work better.
Yes there are other treatments but for PD patients light therapy is probably the safest and most direct as it will let your body create the balance.
We should have posted this earlier but one of us was in denial about having SAD.
 One last area to discuss when speaking about depression is Seasonal Affective Disorder - SAD.
One last area to discuss when speaking about depression is Seasonal Affective Disorder - SAD.It isn't just the winter blues because you feel cooped in even when you have to go out and about. SAD is more serious than that. It affects patients and caregivers alike. Some people have SAD even in the spring and summer. And treatment can be the same for everyone.
Winter SAD symptoms:
Weight gain
Carb cravings
Oversleeping - waking too early
Indecisiveness
Decreased sex drive
Apathy
Feelings of hopelessness
Anxiety
Suicidal thoughts
Lack of concentration or difficulty concentrating
Difficulty processing information
Summer-Spring SAD symptoms:
Anxiety
Insomnia
Irritability
Agitation
Loss of appetite
Weight loss
Increased sex drive
Yes there is even Reverse SAD which involves manic symptoms which makes sense when you think about it. Symptoms include hypperactivity, increased social activity, extreme enthusiasm, persistent UP mood.
 For roughly 80 percent of SAD sufferers, melatonin levels peak just when it’s time to wake up. For those people, morning light therapy is best. For others, melatonin drops too soon, and they find themselves waking up in the middle of the night. Those patients may find that evening light therapy can work better.
For roughly 80 percent of SAD sufferers, melatonin levels peak just when it’s time to wake up. For those people, morning light therapy is best. For others, melatonin drops too soon, and they find themselves waking up in the middle of the night. Those patients may find that evening light therapy can work better.Why does SAD occur? And why would PD patients be likely to have SAD?
Because many older PD patients home-bind themselves, it is quite likely that their vitamin D levels as well as melatonin level drop as their exposure to natural sunlight is reduced. SAD is circadian in that it is a winter disorder. Less sunlight means decreased melatonin. Melatonin, a powerful anti-oxidant and free radical scavenger, has been shown to provide neuroprotection in PD. This endocrine plays a part in the biologic regulation of circadian rhythms, of mood and sleep.
Difference between sleeping in summer and winter:
Summer=wake to sun/sleep when dark
Winter=wake in dark/sleep in dark
Lack of sunlight=reduced melatonin
Other influences of the neurotransmitters
Stress=reduced serotonin
Lack of sleep=reduced serotonin
Lack of activity/boredom=reduced dopamine/norepinephrine
Poor nutrition (lack of the stress vitamins B6, C and E)=reduced serotonin
and by the way, deionized air=reduced serotonin - summer produces more negative ions.
SAD symptoms:
Weight gain
Carb craving
Oversleeping
Indecisiveness
Decreased sex drive
Apathy
Anxiety
Suicidal thoughts
Lack of concentration-difficulty focusing
The treatment for SAD is sitting in front of a light box or lamp for at least 1/2 hour a day- an hour if necessary. An alternative is a dawn light which simulates sunrise as it gradually brightens. In bright light therapy the light is usually a full spectrum light 10,000-25,000 lux. Although treatment is done with the eyes open, one should not be looking at the light. There are also blue lights which can be used.
My sister had another idea. She has replaced the bulbs in her kitchen fixures with full spectrum bulbs. The only problem with doing this is that for most people the treatment should be done in the morning and the lights in her kitchen are rarely on before dark.
I would suggest having breakfast or morning coffee in front of the light or under it. There are bulbs available so that you would only need a lamb with the shade removed or one that you can tilt in your direction. Perhaps a lamp could be set up next to the computer monitor for your morning read of email and news. This way you are not squeezing in yet another therapy but rather multi-tasking in an easy way.
bulbs available so that you would only need a lamb with the shade removed or one that you can tilt in your direction. Perhaps a lamp could be set up next to the computer monitor for your morning read of email and news. This way you are not squeezing in yet another therapy but rather multi-tasking in an easy way.
Because many older PD patients home-bind themselves, it is quite likely that their vitamin D levels as well as melatonin level drop as their exposure to natural sunlight is reduced. SAD is circadian in that it is a winter disorder. Less sunlight means decreased melatonin. Melatonin, a powerful anti-oxidant and free radical scavenger, has been shown to provide neuroprotection in PD. This endocrine plays a part in the biologic regulation of circadian rhythms, of mood and sleep.
Difference between sleeping in summer and winter:
Summer=wake to sun/sleep when dark
Winter=wake in dark/sleep in dark
Lack of sunlight=reduced melatonin
Other influences of the neurotransmitters
Stress=reduced serotonin
Lack of sleep=reduced serotonin
Lack of activity/boredom=reduced dopamine/norepinephrine
Poor nutrition (lack of the stress vitamins B6, C and E)=reduced serotonin
and by the way, deionized air=reduced serotonin - summer produces more negative ions.
SAD symptoms:
Weight gain
Carb craving
Oversleeping
Indecisiveness
Decreased sex drive
Apathy
Anxiety
Suicidal thoughts
Lack of concentration-difficulty focusing
The treatment for SAD is sitting in front of a light box or lamp for at least 1/2 hour a day- an hour if necessary. An alternative is a dawn light which simulates sunrise as it gradually brightens. In bright light therapy the light is usually a full spectrum light 10,000-25,000 lux. Although treatment is done with the eyes open, one should not be looking at the light. There are also blue lights which can be used.
My sister had another idea. She has replaced the bulbs in her kitchen fixures with full spectrum bulbs. The only problem with doing this is that for most people the treatment should be done in the morning and the lights in her kitchen are rarely on before dark.
I would suggest having breakfast or morning coffee in front of the light or under it. There are
 bulbs available so that you would only need a lamb with the shade removed or one that you can tilt in your direction. Perhaps a lamp could be set up next to the computer monitor for your morning read of email and news. This way you are not squeezing in yet another therapy but rather multi-tasking in an easy way.
bulbs available so that you would only need a lamb with the shade removed or one that you can tilt in your direction. Perhaps a lamp could be set up next to the computer monitor for your morning read of email and news. This way you are not squeezing in yet another therapy but rather multi-tasking in an easy way. Yes there are other treatments but for PD patients light therapy is probably the safest and most direct as it will let your body create the balance.
We should have posted this earlier but one of us was in denial about having SAD.
Friday, March 13, 2009
Questions About Parkinson's Disease Part V - Depression & PD
Parkinson's Depression and the three molecules of depression: serotonin, norepinephrine and dopamine
Depression is a common problem for many people - we hear those ads on television every day along with the side effect warnings. Parkinson's patients, their families and caregivers alike may go through periods of depression. The remedies and treatments for PDer and the carer may differ because of medication and supplement interactions and the disease itself.
Some research has indicated that the chemical changes in the brain caused by depression might actually be a trigger for PD. We know that Parkinson's shows itself after a significant loss of the neurotransmitters dopamine and norepinephrine; is serotonin deficiency occurring at the same time or earlier? One view is that synaptic depletion of serotonin allows a fall in norepinephrine levels. Which might mean that manipulating serotonin levels would increase norepinephrine levels if the norepinephrine depletion hadn't occurred because of the dopamine depletion. Which is why depression treatment can be different in Parkinson's disease.
Depression is often one of the 1st symptoms of PD - long before any obvious ones. Older patients can also manifest confusion, memory loss and apathy. PD is not the only disease associated with depression; Alzheimer's disease, kidney failure, stroke, AIDS, chronic fatigue, fibromyalgia, cancer and hypothyroidism patients also suffer from depression.
The PD symptoms for depression range from lack of energy, a struggle to arise to begin the new day, sleep disturbances, feeling irritable and anxious, have a sense of the loss of self-worth, feeling of self-guilt and loss of appetite. Because depression often manifests early it may seem to everyone that it is an extension of the appearance of Parkinson's Disease symptoms and the diagnosis. The depression may come and go. In the late stages depression may actually be caused by a chemical imbalance.
It is understandable that people would be depressed by having any disease because there is the shock, the grief and the sometimes not so subtle physical changes. There are differences in PD. A primary difference is that the depression over loss of mobility and appearance of other motor symptoms may actually acerbate the symptoms.
Psychological therapy such as cognitive-behavioral therapy as opposed to psychotherapy can be of benefit to PD patients because it can help restore a more positive self image which can assist in improving caregiver and family relations as well. It can also help the patient focus on problem-solving rather than the loss.
There are also medications which help. Be aware, however, the Cleveland Clinic information suggested that amoxipine (Ascendin) can make PD symptoms worse. And there are others which can cause low blood pressure. Selective serotonin uptake inhibitors (SSRIs) are among the more recent, safer meds. However, recent a study showed that nortriptyline, a tricyclic antidepressant (TCA) which targets both serotonin and norepinephrine receptors was more effective in PD patients than paroxetine (Paxil) an SSRI. Tricyclics are older antidepressants which must be monitored closely for overdose
If you are taking Zelapar or Zydis selegiline, Eldepryl, Cipro (Ciprofloxacin) there are cautions about taking antidepressants, SSRIs and tricyclic antidepressants because of interactions and side effects. Prozac and Zoloft may cause anxiety, tremor and insomnia.
Much to our surprise, we read that electroconvulsive therapy ("shock" therapy) works more rapidly than medication and may actually help improve other PD symptoms in some cases.
Another important treatment is exercise. It will help both the the depression and the PD symptoms.
There are also supplements which can help. Remember that medications are not the only substances which can cause side effects. Food and dietary supplements also have side effects.
Most of us are familiar with St John's Wort. You can also find St John's Wort in combination with 5-HTP and vitamin B-6. L-5-Hydroxytryptophan crosses the blood brain barrier and is said to help relieve anxiety and depression as well as being a natural relaxant which also aids in insomnia. There is some evidence that 5-HTP should not be used with carbidopa. If you are taking Azilect, if you are combining with MAO1 inhibitors, you should make sure to consult your doctor before taking ST John's Wort or 5-HTP. (Currently Teva, manufacturer of Azilect, is working with the FDA to change the description to MAO-B inhibitor which can be more broadly prescribed.)
Because of the impact upon the three molecules, the big 3 monoamines of Parkinson's, it is important to discuss any supplements you are considering with your neurologist. Melatonin is another supplement which is used in low doses to treat depression because it is known to raise serotonin levels and to help adjust the sleep cycle. Supplements should not be taken without a discussion with your physician.
It is important to keep in mind that everything you take into your body, including the foods you eat, will interact with everything else you take. Some combinations are synergistic, they work well together and may amplify the benefits while combining others can cause serious side effects.
One last area to discuss is Seasonal Affective Disorder - SAD.
It isn't just the winter blues because you feel cooped in even when you have to go out and about. SAD is more serious than that. It affects patients and caregivers alike. Some people have SAD even in the spring and summer.
Depression is a common problem for many people - we hear those ads on television every day along with the side effect warnings. Parkinson's patients, their families and caregivers alike may go through periods of depression. The remedies and treatments for PDer and the carer may differ because of medication and supplement interactions and the disease itself.
Some research has indicated that the chemical changes in the brain caused by depression might actually be a trigger for PD. We know that Parkinson's shows itself after a significant loss of the neurotransmitters dopamine and norepinephrine; is serotonin deficiency occurring at the same time or earlier? One view is that synaptic depletion of serotonin allows a fall in norepinephrine levels. Which might mean that manipulating serotonin levels would increase norepinephrine levels if the norepinephrine depletion hadn't occurred because of the dopamine depletion. Which is why depression treatment can be different in Parkinson's disease.
Depression is often one of the 1st symptoms of PD - long before any obvious ones. Older patients can also manifest confusion, memory loss and apathy. PD is not the only disease associated with depression; Alzheimer's disease, kidney failure, stroke, AIDS, chronic fatigue, fibromyalgia, cancer and hypothyroidism patients also suffer from depression.
The PD symptoms for depression range from lack of energy, a struggle to arise to begin the new day, sleep disturbances, feeling irritable and anxious, have a sense of the loss of self-worth, feeling of self-guilt and loss of appetite. Because depression often manifests early it may seem to everyone that it is an extension of the appearance of Parkinson's Disease symptoms and the diagnosis. The depression may come and go. In the late stages depression may actually be caused by a chemical imbalance.
It is understandable that people would be depressed by having any disease because there is the shock, the grief and the sometimes not so subtle physical changes. There are differences in PD. A primary difference is that the depression over loss of mobility and appearance of other motor symptoms may actually acerbate the symptoms.
Psychological therapy such as cognitive-behavioral therapy as opposed to psychotherapy can be of benefit to PD patients because it can help restore a more positive self image which can assist in improving caregiver and family relations as well. It can also help the patient focus on problem-solving rather than the loss.
There are also medications which help. Be aware, however, the Cleveland Clinic information suggested that amoxipine (Ascendin) can make PD symptoms worse. And there are others which can cause low blood pressure. Selective serotonin uptake inhibitors (SSRIs) are among the more recent, safer meds. However, recent a study showed that nortriptyline, a tricyclic antidepressant (TCA) which targets both serotonin and norepinephrine receptors was more effective in PD patients than paroxetine (Paxil) an SSRI. Tricyclics are older antidepressants which must be monitored closely for overdose
If you are taking Zelapar or Zydis selegiline, Eldepryl, Cipro (Ciprofloxacin) there are cautions about taking antidepressants, SSRIs and tricyclic antidepressants because of interactions and side effects. Prozac and Zoloft may cause anxiety, tremor and insomnia.
Much to our surprise, we read that electroconvulsive therapy ("shock" therapy) works more rapidly than medication and may actually help improve other PD symptoms in some cases.
Another important treatment is exercise. It will help both the the depression and the PD symptoms.
There are also supplements which can help. Remember that medications are not the only substances which can cause side effects. Food and dietary supplements also have side effects.
Most of us are familiar with St John's Wort. You can also find St John's Wort in combination with 5-HTP and vitamin B-6. L-5-Hydroxytryptophan crosses the blood brain barrier and is said to help relieve anxiety and depression as well as being a natural relaxant which also aids in insomnia. There is some evidence that 5-HTP should not be used with carbidopa. If you are taking Azilect, if you are combining with MAO1 inhibitors, you should make sure to consult your doctor before taking ST John's Wort or 5-HTP. (Currently Teva, manufacturer of Azilect, is working with the FDA to change the description to MAO-B inhibitor which can be more broadly prescribed.)
Because of the impact upon the three molecules, the big 3 monoamines of Parkinson's, it is important to discuss any supplements you are considering with your neurologist. Melatonin is another supplement which is used in low doses to treat depression because it is known to raise serotonin levels and to help adjust the sleep cycle. Supplements should not be taken without a discussion with your physician.
It is important to keep in mind that everything you take into your body, including the foods you eat, will interact with everything else you take. Some combinations are synergistic, they work well together and may amplify the benefits while combining others can cause serious side effects.
One last area to discuss is Seasonal Affective Disorder - SAD.
It isn't just the winter blues because you feel cooped in even when you have to go out and about. SAD is more serious than that. It affects patients and caregivers alike. Some people have SAD even in the spring and summer.
We'll talk more about SAD in the next post - better late than never.
Thursday, March 12, 2009
Google Founder Gives PD Patients Opportunity for Easy Genetic Testing
Genetic Research Opportunity for Parkinson's Disease Patients
23andMe, Inc a personal genetic company together with the Michael J Fox Foundation (MJFF) and The Parkinson's Institute and Clinical Center (PI) announced on March 12th, 2009 that it was launching an initiative program in which it will enroll 10,000 individuals with Parkinson's disease on a first come - first served basis in a research program which will allow online information gathering about patients with the genotyping of participants.
Although the cost for such a program is normally $399.00, the program has been underwritten by Google co-founder Sergey Brin whose mother has PD. Mr Brin discovered through 23andMe that he has a genetic disposition for Parkinson's. The cost to participants through either MJFF or PI will be only $25.00.
For those who want to be a part of this wonderful opportunity, you can enroll at the Michael J Fox Foundation website:
To link to the press release by MJFF:
To link to the full press release with additional information:
Addendum: The study may still be open, so even though it is 2010, you may not be too late - it is certainly worth a click or two.
23andMe, Inc a personal genetic company together with the Michael J Fox Foundation (MJFF) and The Parkinson's Institute and Clinical Center (PI) announced on March 12th, 2009 that it was launching an initiative program in which it will enroll 10,000 individuals with Parkinson's disease on a first come - first served basis in a research program which will allow online information gathering about patients with the genotyping of participants.
Although the cost for such a program is normally $399.00, the program has been underwritten by Google co-founder Sergey Brin whose mother has PD. Mr Brin discovered through 23andMe that he has a genetic disposition for Parkinson's. The cost to participants through either MJFF or PI will be only $25.00.
For those who want to be a part of this wonderful opportunity, you can enroll at the Michael J Fox Foundation website:
To link to the press release by MJFF:
To link to the full press release with additional information:
Addendum: The study may still be open, so even though it is 2010, you may not be too late - it is certainly worth a click or two.
Wednesday, March 11, 2009
Questions About Parkinson's Disease - part IV
MDS-UPDRS Table
Part I Non-Motor Aspects of Daily Living | Part II Motor Experiences of Daily Living | Part III Motor Examination Entire Body | Part IV Motor Complications: Dyskinesias and Fluctuations |
| Cognitive impairment | Speech | Speech | Time spent with dyskinesias (involuntray movement) |
| Hallucinations and psychosis | Saliva and Swallowing | Facial expression | functional impact of dyskinesias |
| Depressed mood | Eating tasks | Rigidity | painful off-state dystonia (levadopa decrement) |
| Anxious Mood | Dressing | Hand Movements | Motor fluctuations in off-state |
| Apathy | Hygiene | Rapid alternating movements of hands (pronation-supination) | Functional impact of motor fluctuations |
| Features of dopamine dysregulation | Handwriting | Toe tapping | Complexity of motor fluctuations |
| Sleep problems | Performing hobbies and other activities | leg agility | - |
| Daytime sleepiness | Turning in bed | Rising from a chair | - |
| Pain & other sensations | Tremor impact on activities | Gait | - |
| Urinary problems | Getting in and out of bed | Freezing of gait | - |
| Constipation problems | Walking and balancing | Posture | - |
| Lightheadedness on standing | Freezing | Global spontaniety of movement (body bradykinesia) | - |
| Fatigue | - | Postural hand tremor | - |
| - | - | Kinetic hand tremor | - |
| - | - | Rest tremor amplitude | - |
| - | - | Constancy of rest tremor | - |
Questions About Parkinson's Disease - Part III
Parkinson's Disease measurement scales for diagnoses and disease progression
Most of us have seen the rating scales for PD before. These are still a very significant part of the Parkinson's diagnosis and the progression tracking throughout the path of this disease. We list the Hohen and Yahr (HY) scale first because it is a way to evaluate motor impairment as well as physical disability. It also can be used to measure response to treatment.
The Unified Parkinson's Disease Rating Scale, known as the UPDRS is used to provide an assessment means for diagnosis and response to treatment. The UPDRS was revised under the sponsorship of The Movement Disorder Society. It is now known as the MDS-UPDRS. We have provided a table of areas for the MDS-UPDRS as well as links to the older and newer versions in html and PDF formats which list the measurements and the scoring. It was recently revised to be more user-friendly to patients, caregivers and diagnosticians. It appears to be getting some good reviews.
The Schwab and England Activities of Daily Living Scale should be read by family, caregivers and patients alike.
For the just curious, these scales should provide some instant recognition of Parkinson's Disease and the daily life of people with PD and their families.
Most of us have seen the rating scales for PD before. These are still a very significant part of the Parkinson's diagnosis and the progression tracking throughout the path of this disease. We list the Hohen and Yahr (HY) scale first because it is a way to evaluate motor impairment as well as physical disability. It also can be used to measure response to treatment.
The Unified Parkinson's Disease Rating Scale, known as the UPDRS is used to provide an assessment means for diagnosis and response to treatment. The UPDRS was revised under the sponsorship of The Movement Disorder Society. It is now known as the MDS-UPDRS. We have provided a table of areas for the MDS-UPDRS as well as links to the older and newer versions in html and PDF formats which list the measurements and the scoring. It was recently revised to be more user-friendly to patients, caregivers and diagnosticians. It appears to be getting some good reviews.
The Schwab and England Activities of Daily Living Scale should be read by family, caregivers and patients alike.
For the just curious, these scales should provide some instant recognition of Parkinson's Disease and the daily life of people with PD and their families.
Hohen and Yahr Scale
Stage one: Mild inconvenient symptoms on one side of the body
only. May present as tremor in one limb
Friends may notice changes in posture,
walking, facial expression
Stage two: Symptoms on both sides of the body.
Minimal impairment of balance.
Posture and gait affected
Stage three: Balance impairment. Mild to moderate disease.
Physically independent.
Generalized and moderately severe dysfunction
Stage four: Severe disability, but may still be able to walk or stand
Stiffness and bradykinesia, although tremor may lessen
No longer able to live independently .
Stage five: Wheelchair-bound or bedridden unless assisted
Loss of weight and muscle mass
Requires constant nursing care
only. May present as tremor in one limb
Friends may notice changes in posture,
walking, facial expression
Stage two: Symptoms on both sides of the body.
Minimal impairment of balance.
Posture and gait affected
Stage three: Balance impairment. Mild to moderate disease.
Physically independent.
Generalized and moderately severe dysfunction
Stage four: Severe disability, but may still be able to walk or stand
Stiffness and bradykinesia, although tremor may lessen
No longer able to live independently .
Stage five: Wheelchair-bound or bedridden unless assisted
Loss of weight and muscle mass
Requires constant nursing care
Movement Disorder Society MDS-UPDRS New version
Chairperson: Christopher G Goetz
Chairperson: Christopher G Goetz
MDS-UPDRS pdf format
UPDRS - Unified Parkinson's Disease Rating Scale
Old version pdf format
Old version pdf format
Schwab and England Activities of Daily Living Scale (ADL)
100% -Completely independent. Able to do all chores without slowness, difficulty or impairment.
90% - Completely independent. Able to do all chores with some slowness, difficulty or impairment.
May take twice as long to complete.
80% - Independent in most chores. Takes twice as long. Conscious of difficulty and slowing
70% - Not completely independent. More difficulty with chores. 3 to 4 times longer to complete chores for some.
May take large part of day for chores.
60% - Some dependency. Can do most chores, but very slowly and with much effort. Errors, some impossible
50% - More dependent. Help with 1/2 of chores. Difficulty with everything
40% - Very dependent. Can assist with all chores but few alone
30% - With effort, now and then does a few chores alone or begins alone. Much help needed
20% - Nothing alone. Can do some slight help with some chores. Severe invalid state
10% - Totally dependent, helpless
0% - Vegetative functions such as swallowing, bladder/bowel function are not functioning. Bedridden
In Part V it will be time to talk about the diagnosis and treatments for Parkinson's Disease and depression
In Part V it will be time to talk about the diagnosis and treatments for Parkinson's Disease and depression
Monday, March 9, 2009
President Obama Bans the Ban
Removal of Embryonic Stem Cell Ban Gives Hope for Cures

I don't know about you but in this house we
feel like the Munchkins singing when Dorothy's house fell on the Wicked Witch of the East. It isn't because we are positive that stem cells will hold a cure for Parkinson's disease, although we are pretty sure that many conditions will find a resolution as a result of research in this area. It is because we feel that we have been pulled from the dark age cycle of provincial mentality. The USA can reenter an age of competitive research internationally.
President Obama issued an executive order to lift the Bush ban on Federal support for embryonic stem cell research. While scientists say stem cell research will lead to many medical breakthroughs, many religious groups oppose the research. The awful irony is that the readily available embryonic stem cells which were so protected were never going to be used. They became part of a confused, misguided, mean-spirited religious and political processional to the trash pile. And the life potential of so many people who will perish because a cure hasn't been found in time became just another ignored member...until now.
Obama promised to "vigorously support" new research. The Bush ban had prevented federal funding for any research on embryonic stem cells created after August 2001. Obama is showing that his administration is not going to allow the political and religious interference into scientific research that has frustrated sufferers of chronic diseases for the last 8 years. Neurological Diseases such as Parkinson's, Multiple Sclerosis (MS), ALS, Type 1 Diabetes, Duchenne and Becker Muscular Dystrophy (DMD and BMD) might have have been far closer to a cure without Bush's simplistic interference.
Now that the executive order is issued the National Institutes Of Health will need about a year to rewrite the regulations and guide lines, before federally funded ESC research can begin again.
Join us in reading the entire Executive Order
http://www.whitehouse.gov/the_press_office/Removing-Barriers-to-Responsible-Scientific-Research-Involving-Human-Stem-Cells/

I don't know about you but in this house we
feel like the Munchkins singing when Dorothy's house fell on the Wicked Witch of the East. It isn't because we are positive that stem cells will hold a cure for Parkinson's disease, although we are pretty sure that many conditions will find a resolution as a result of research in this area. It is because we feel that we have been pulled from the dark age cycle of provincial mentality. The USA can reenter an age of competitive research internationally.
President Obama issued an executive order to lift the Bush ban on Federal support for embryonic stem cell research. While scientists say stem cell research will lead to many medical breakthroughs, many religious groups oppose the research. The awful irony is that the readily available embryonic stem cells which were so protected were never going to be used. They became part of a confused, misguided, mean-spirited religious and political processional to the trash pile. And the life potential of so many people who will perish because a cure hasn't been found in time became just another ignored member...until now.
Obama promised to "vigorously support" new research. The Bush ban had prevented federal funding for any research on embryonic stem cells created after August 2001. Obama is showing that his administration is not going to allow the political and religious interference into scientific research that has frustrated sufferers of chronic diseases for the last 8 years. Neurological Diseases such as Parkinson's, Multiple Sclerosis (MS), ALS, Type 1 Diabetes, Duchenne and Becker Muscular Dystrophy (DMD and BMD) might have have been far closer to a cure without Bush's simplistic interference.
Now that the executive order is issued the National Institutes Of Health will need about a year to rewrite the regulations and guide lines, before federally funded ESC research can begin again.
Join us in reading the entire Executive Order
http://www.whitehouse.gov/the_press_office/Removing-Barriers-to-Responsible-Scientific-Research-Involving-Human-Stem-Cells/
Friday, March 6, 2009
Questions About Parkinson's Disease - Part II
Questions about Parkinson's Disease Symptoms & Diagnosis Part II
Welcome to the second of the Questions about Parkinson's Disease evoloved from a questionnaire submitted by a young student a few days ago.
The Questionnaire
How old were you when you received your PD diagnosis? I have been diagnosed with PD for 6 years. I am now 67. I was aware of symptoms for at least 8 years and my wife was aware of some of my symptoms for several years before that. She did not have a name to go with the symptoms however because she as well as my doctors did not know the early symptoms. By the time a patient is diagnosed the dopamine and norepinephrine levels have already dropped by 60 to 80%. (Serontonin levels and dopamine levels are supposed to be in balance.)
What are the first signs and symptoms of Parkinson's disease? The symptoms can vary from person to person. Stiffness, tremors, balance, walking gait (slow, shuffle) These are also symptoms used in the clinical diagnosis. Loss of sense of smell is an early sign which is not yet widely recognized by internists. It is often one of the earliest signs.
What are the characteristic symptoms of Parkinson's disease? The University of Maryland uses the acronym TRAP: Tremor, Rigidity, Akinesia (lack of movement) Postural instability
Are there other symptoms? Yes, there are secondary symptoms which like the primary symptoms may not occur in every patient.
Stooped posture - a tendency to lean forward
Dystonia - Prolonged muscle contraction causing repetitive movements, twisting
Fatigue
Impaired fine motor dexterity and motor coordination
Impaired large motor coordination
Decreased movement of arms such as decreased arm swing-not to be confused with occurrence of tremors
Akathisia - inablilty to "sit still" often caused by antipsychotics
Speech problems such as softness of voice or slurred speech caused by lack of muscle control Lack of facial expression, or "masking"
Micrographia, small, cramped handwriting
Difficulty swallowing, choking
Sexual dysfunction
Drooling
Constipation
Urinary issues
What are the diagnostic tests used to diagnosis Parkinson's disease? There are really not many diagnostic tests for PD. Rather than testing by an internist or GP, usually the diagnosis falls to a neurologist who specializes in neuro-motor problems.
Conversation and physical observation become the major part of the diagnosis because you can't do a biopsy for PD. CAT or PET scans or an MRIs can rule out other conditions but have little definitive value for PD at the diagnostic stage at this time. Nor is an EEG effective because in all of these tests the brain of a PD patient appears normal. What remains is a clinical diagnosis (office diagnosis) based upon a list of symptoms.
The PD diagnostic symptom check list begins with:
Resting tremor
Bradykinesia (slowness of movement)
Rigidity (increased muscle tone-stiffness-inability of the muscle to flex and relax as it is always flexed)
Postural instability (impaired balance and coordination which results difficulty making normal turns, freezing, compensatory posture)
Diagnoses can be missed or incorrect. But symptom progression becomes the validating measure...or not
Some doctors use the questions on a PDRS which is really a disease tracking method. In my case the internist listened to my list of symptoms and then asked a series of questions: look at my finger etc, cognitive questions, standard neurological questions. He then said that he thought that I either had Essential Tremor or Parkinson's Disease and referred my to a neurologist. I do not know if he checked my chart to see if I was taking any meds which block the production of dopamine in the brain but he may have done that.
You can find that list of dopamine blocking meds here: http://www.wemove.org/par/par_dia.html
When I was diagnosed the neurologist gave me some standard neurological tests and an electro-conductivity test of muscles (Electromyography) which involves needles in the arms, legs, and various places on the body. That test is not to determine Parkinson's but rather ALS - it will also rule out ALS in the case of Parkinson's disease. In my case it confirmed that I had carpal tunnel syndrome. Based upon the clinical tests and his judgement, his clinical diagnosis was PD.
He then prescribed Amantadine because I had already told him about taking CoQ10 and that I would not take Sinemet yet. The Amantadine stopped the pinpoint pains which was a relief.
In the future: At this time there is research underway to develop an MRI test for iron in the brain cells. The technology comes from work with the Diamond Synchrotron.
(You can check the synchrotron in Wikipedia http://en.wikipedia.org/wiki/Synchrotron)
How does Parkinson's disease affect your daily life? The disease begins with subtle differences.
Difficulty getting in and out of cars.
Being stiff and unable to bend to do small household repairs.
Certainly not being able to climb a ladder to make larger repairs because my balance and flexibility are affected. (I used to be a contractor and could literally build a house.) So it has changed me from what I could do to not being able to do simple things.
I can still read and think and spend much of my time learning more about Parkinson's research and therapies as well as writing about them.
Getting dressed is more difficult due to stiffness. I have to be careful about what shirts I wear to exercise therapy because I have to be able to put them on and take them off by myself at the therapy center.
Because I have found supplements which help, I no longer have much problem swallowing and choking. My voice is somewhat restored because of taking DynaCirc CR, a calcium channel blocker which crosses the blood brain barrier and may actually have slowed the progression of the Parkinson's disease.
I was very fortunate to have found a doctor who would allow me to take it - of course I had been a cardiac patient before that and he decided to allow it because of the label use although now it is accepted for off-label usage.
What are some complaints that you have with having Parkinson's disease? A disease which can cost your livelihood it not fun. It makes things more difficult to be on a reduced income in a time when plenty of healthy people are competing with you for the same jobs. Although I still have my cognitive skills, it takes me longer.
Because of the stiffness on one side of my body, I have some difficulty typing. Actually we are doing exercises for that and occasionally I am able to return to typing with both hands. I do not like not being able to make repairs around the house, not be able to do yard work. I used to ride my bike for miles. I have not been able to ride my bike for several years because of the stiffness (and the pain in my knees.)
I never liked taking any pills and now I have to take meds (heart and PD) as well as many supplements which support the treatment. I finally realized, when I added the last supplement, that it was time to make a chart of what to take when.
The problem with having a chronic disease for which there is no cure is that you can read about research and therapies but the process takes a long time. There is a lot of trial and error to find correct directions. Research is very expensive and the FDA makes it very very expensive to get approval.
I feel that after Phase I clinical trials a drug should be offered to the public as long as patients agreed not to sue if there were unexpected side effects. (My wife has mixed feelings about that) But only an act of Congress could get that enacted and there has been a long history of not being able to act in the interests of disease minorities and mixing religion with politics - antithetical to the founding principles of this country but nonetheless present now as it has been throughout history.
You get used to people laughing at the way you move or at least I did - I guess some people just don't go out much because of that.
What changes did you manifest when Parkinson's disease became very bad? I have not reached the "very bad" stage and with some luck and by continuing to use the medication, supplements, exercise, massage therapies I am using, I hope that I will progress very slowly to the next stage...if at all. If I can remain in stage 2 long enough, perhaps I can live long enough to see a cure.
If by very bad you mean when did I see a doctor, I will explain the early symptoms and what took me to the doctor's office for a medical diagnosis.
Understand that by the time I went to the doctor, I was pretty sure that I knew what I had and had already begun to take the antioxidant CoQ10 which actually was helping me. My early symptoms were foot drag - which I had had for a few years but attributed to the arthritis triggered by walking on very hard floors at work; loss of sense of smell which had been steadily going for several years, stiffness which made it difficult to get in and out of cars, some depression which I didn't acknowledge much, a tremor which began in my left thumb, and small pinpoint sized powerful pain in my torso and later anywhere on my body - this made me think that there was something neurologically wrong with me and that is why I made the appointment.
Welcome to the second of the Questions about Parkinson's Disease evoloved from a questionnaire submitted by a young student a few days ago.
The Questionnaire
How old were you when you received your PD diagnosis? I have been diagnosed with PD for 6 years. I am now 67. I was aware of symptoms for at least 8 years and my wife was aware of some of my symptoms for several years before that. She did not have a name to go with the symptoms however because she as well as my doctors did not know the early symptoms. By the time a patient is diagnosed the dopamine and norepinephrine levels have already dropped by 60 to 80%. (Serontonin levels and dopamine levels are supposed to be in balance.)
What are the first signs and symptoms of Parkinson's disease? The symptoms can vary from person to person. Stiffness, tremors, balance, walking gait (slow, shuffle) These are also symptoms used in the clinical diagnosis. Loss of sense of smell is an early sign which is not yet widely recognized by internists. It is often one of the earliest signs.
What are the characteristic symptoms of Parkinson's disease? The University of Maryland uses the acronym TRAP: Tremor, Rigidity, Akinesia (lack of movement) Postural instability
Are there other symptoms? Yes, there are secondary symptoms which like the primary symptoms may not occur in every patient.
Stooped posture - a tendency to lean forward
Dystonia - Prolonged muscle contraction causing repetitive movements, twisting
Fatigue
Impaired fine motor dexterity and motor coordination
Impaired large motor coordination
Decreased movement of arms such as decreased arm swing-not to be confused with occurrence of tremors
Akathisia - inablilty to "sit still" often caused by antipsychotics
Speech problems such as softness of voice or slurred speech caused by lack of muscle control Lack of facial expression, or "masking"
Micrographia, small, cramped handwriting
Difficulty swallowing, choking
Sexual dysfunction
Drooling
Constipation
Urinary issues
What are the diagnostic tests used to diagnosis Parkinson's disease? There are really not many diagnostic tests for PD. Rather than testing by an internist or GP, usually the diagnosis falls to a neurologist who specializes in neuro-motor problems.
Conversation and physical observation become the major part of the diagnosis because you can't do a biopsy for PD. CAT or PET scans or an MRIs can rule out other conditions but have little definitive value for PD at the diagnostic stage at this time. Nor is an EEG effective because in all of these tests the brain of a PD patient appears normal. What remains is a clinical diagnosis (office diagnosis) based upon a list of symptoms.
The PD diagnostic symptom check list begins with:
Resting tremor
Bradykinesia (slowness of movement)
Rigidity (increased muscle tone-stiffness-inability of the muscle to flex and relax as it is always flexed)
Postural instability (impaired balance and coordination which results difficulty making normal turns, freezing, compensatory posture)
Diagnoses can be missed or incorrect. But symptom progression becomes the validating measure...or not
Some doctors use the questions on a PDRS which is really a disease tracking method. In my case the internist listened to my list of symptoms and then asked a series of questions: look at my finger etc, cognitive questions, standard neurological questions. He then said that he thought that I either had Essential Tremor or Parkinson's Disease and referred my to a neurologist. I do not know if he checked my chart to see if I was taking any meds which block the production of dopamine in the brain but he may have done that.
You can find that list of dopamine blocking meds here: http://www.wemove.org/par/par_dia.html
When I was diagnosed the neurologist gave me some standard neurological tests and an electro-conductivity test of muscles (Electromyography) which involves needles in the arms, legs, and various places on the body. That test is not to determine Parkinson's but rather ALS - it will also rule out ALS in the case of Parkinson's disease. In my case it confirmed that I had carpal tunnel syndrome. Based upon the clinical tests and his judgement, his clinical diagnosis was PD.
He then prescribed Amantadine because I had already told him about taking CoQ10 and that I would not take Sinemet yet. The Amantadine stopped the pinpoint pains which was a relief.
In the future: At this time there is research underway to develop an MRI test for iron in the brain cells. The technology comes from work with the Diamond Synchrotron.
(You can check the synchrotron in Wikipedia http://en.wikipedia.org/wiki/Synchrotron)
How does Parkinson's disease affect your daily life? The disease begins with subtle differences.
Difficulty getting in and out of cars.
Being stiff and unable to bend to do small household repairs.
Certainly not being able to climb a ladder to make larger repairs because my balance and flexibility are affected. (I used to be a contractor and could literally build a house.) So it has changed me from what I could do to not being able to do simple things.
I can still read and think and spend much of my time learning more about Parkinson's research and therapies as well as writing about them.
Getting dressed is more difficult due to stiffness. I have to be careful about what shirts I wear to exercise therapy because I have to be able to put them on and take them off by myself at the therapy center.
Because I have found supplements which help, I no longer have much problem swallowing and choking. My voice is somewhat restored because of taking DynaCirc CR, a calcium channel blocker which crosses the blood brain barrier and may actually have slowed the progression of the Parkinson's disease.
I was very fortunate to have found a doctor who would allow me to take it - of course I had been a cardiac patient before that and he decided to allow it because of the label use although now it is accepted for off-label usage.
What are some complaints that you have with having Parkinson's disease? A disease which can cost your livelihood it not fun. It makes things more difficult to be on a reduced income in a time when plenty of healthy people are competing with you for the same jobs. Although I still have my cognitive skills, it takes me longer.
Because of the stiffness on one side of my body, I have some difficulty typing. Actually we are doing exercises for that and occasionally I am able to return to typing with both hands. I do not like not being able to make repairs around the house, not be able to do yard work. I used to ride my bike for miles. I have not been able to ride my bike for several years because of the stiffness (and the pain in my knees.)
I never liked taking any pills and now I have to take meds (heart and PD) as well as many supplements which support the treatment. I finally realized, when I added the last supplement, that it was time to make a chart of what to take when.
The problem with having a chronic disease for which there is no cure is that you can read about research and therapies but the process takes a long time. There is a lot of trial and error to find correct directions. Research is very expensive and the FDA makes it very very expensive to get approval.
I feel that after Phase I clinical trials a drug should be offered to the public as long as patients agreed not to sue if there were unexpected side effects. (My wife has mixed feelings about that) But only an act of Congress could get that enacted and there has been a long history of not being able to act in the interests of disease minorities and mixing religion with politics - antithetical to the founding principles of this country but nonetheless present now as it has been throughout history.
You get used to people laughing at the way you move or at least I did - I guess some people just don't go out much because of that.
What changes did you manifest when Parkinson's disease became very bad? I have not reached the "very bad" stage and with some luck and by continuing to use the medication, supplements, exercise, massage therapies I am using, I hope that I will progress very slowly to the next stage...if at all. If I can remain in stage 2 long enough, perhaps I can live long enough to see a cure.
If by very bad you mean when did I see a doctor, I will explain the early symptoms and what took me to the doctor's office for a medical diagnosis.
Understand that by the time I went to the doctor, I was pretty sure that I knew what I had and had already begun to take the antioxidant CoQ10 which actually was helping me. My early symptoms were foot drag - which I had had for a few years but attributed to the arthritis triggered by walking on very hard floors at work; loss of sense of smell which had been steadily going for several years, stiffness which made it difficult to get in and out of cars, some depression which I didn't acknowledge much, a tremor which began in my left thumb, and small pinpoint sized powerful pain in my torso and later anywhere on my body - this made me think that there was something neurologically wrong with me and that is why I made the appointment.
These are some of the problem issues of the early stages of advanced Parkinson's disease:
Cognitive decline
Behavioral problems
Communication
Difficulty with urination
Falls
Impaired performance of activities of daily living
Sexual dysfunction
Swallowing
Walking and balance problems
Weight loss
While these problems may occur at any stage, they can become more pronounced in advanced stages. It is a matter of degree.
If you don't mind me asking, what type of health-medical insurance do you have? Originally the health provider was Kaiser Permanente which I had through work. Finding a set of doctors was fairly easy although not all were versed in Parkinson's and my husband had to do most of the information searching on his own. We are now using Aetna Plus Medicare. Unlike the Kaiser HMO, it does not appear to cover as many alternative therapies while Kaiser was limited but some of that is a grey area since I am new to the plan.
Many of the medical expenses associated with the right kind of treatment for Parkinson's are not covered by our insurance since they involve massage therapy, exercise therapy, swim therapy, expensive supplements. Much of our income goes to PD expenses.
Questions about Parkinson's Disease
.jpg) Introduction to Questions about Parkinson's Disease
Introduction to Questions about Parkinson's DiseaseEarlier this week we received some questions from a student who was working on a project for school. Since it's easier to create a questionnaire when you already know the answers, we've revised the question list and are presenting it here with the introductory remarks we also provided.
Introduction Please understand that this patient is only in between phase 1 and 2 and hopefully with the help of the medications he is taking and the addition of supplements and physical-type therapy, we will be able to hold the PD where it is now for awhile. You should know that each patient will manifest symptoms in a slightly different way; certain symptoms may never appear in some patients. Some patients progress rapidly from stage to stage.
Advanced stage PD patients might not be able to answer your questions. At that point you might need to talk to the caregiver and even they might not be able to answer precisely for obvious reason that they are not in the mind of the patient. By this time dopamine levels in the brain have fallen so severely that the remaining neurotransmitter cells cannot function well enough to prevent contracture of the limbs and sometimes the torso. This is more common in patients with psychosis. At the advanced stage the dopamine auto-receptors do not seem to be functioning much if at all.
Another thing you should know is that there are usually undiagnosed precursor symptoms - symptoms which appear well before the standard identifiable symptoms of Parkinson's disease. These symptoms are not identified by either the patient or the physician as being disease related. One school of thought on this is that as the dopamine and subsequently the norepinephrine cells die and their neurotransmitting ceases, the limited dopamine resources are allotted to other body functions. Sense of smell, an early symptom, may be seen by the brain as being peripheral and therefore reduced or shut down.
Depression is another precursor symptom. Being depressed by having the disease is logical but having the depression or severe stress can be either a trigger or an early symptom. PD depression is not treated successfully in the standard ways because the source is different. There are no standardized test for dPD but there are existing depression tests which can be used.
Since Parkinson's, long thought to be an idiopathic disease, may actually be a genetic disease which can skip many generations until it responds to a trigger or a built-in trigger on a mutated gene - there are several associated with PD - it is commonly an older person's disease. The numbers of patients go up at each year over 65. There are also young-onset or early onset patients who manifest differently in many cases. Their response to meds are different also. And sadly there are also juvenile PD patients whose symptoms can manifest between 2 and 20 years of age. The last two groups have not received nearly enough attention in the past.
There are different courses of treatment for patients as some prefer to postpone levadopa medications in favor of levadopa agonists or diet, exercise and supplements. Many of the medications have side effects either short term or within a few years that impact a decision for that line of treatment. There is also some surgery which is about 50% effective in reducing the need for medication. Other courses of treatment include diet, natural supplements and types of physical therapy including exercise therapy, dance therapy, yoga, breathing, voice exercises, swim therapy and massage therapy.
There are different courses of treatment for patients as some prefer to postpone levadopa medications in favor of levadopa agonists or diet, exercise and supplements. Many of the medications have side effects either short term or within a few years that impact a decision for that line of treatment. There is also some surgery which is about 50% effective in reducing the need for medication. Other courses of treatment include diet, natural supplements and types of physical therapy including exercise therapy, dance therapy, yoga, breathing, voice exercises, swim therapy and massage therapy.
Without these extras Steve's body would have stiffened far more than it has already. His massage therapist commented to him that she had never felt shoulders as stiff as his. We are working on that outside the therapy because without regular attention (once a week is not enough but certainly all that we can afford.) I perform a different procedure than the therapist. I was shocked the other day (the day before massage therapy) when his shoulders felt more like a car bumper than what shoulders should feel like. So I improvised and it helped. I did what was intuitive although contrary to what is recommended but it seemed to make a positive difference. I pulled back on his shoulders and then pushed forward against his shoulder blades. Next I moved his upper arms. I would like to say "gently" but it was not gentle. I raised both arms to touch his ears and then alternated with pulling the shoulders forward and back. I also deeply massaged the muscles on either side of his spine followed by moving his upper arms again.
Within the next week we will be making another video of him walking outside (we need space for this) so that we can compare it to videos we made 3 1/2 years ago. Because he also has arthritis in his knees, especially on his weak/stiff side, that has had a profound impact upon his resistance to that pain. The same options for arthritis treatment on knees available to the average person with arthritis are not viable options for a Parkinson's patient.
We have designed other exercises to assist his balance and leg stiffness which affect his ability to walk normally. PD patients often shuffle rather than being able to bend all joints in a normal walk. He has to practice turning by lifting his legs rather than pivoting which aggravates pain in his arthritic knees. We also work on his breathing and his voice. We work on shoulders, arms and arm swing. Again, if you read some of the blog articles or look at the photos, you can see the symptomatic posture with lack of arm swing, difficulty sitting and walking.
He also takes several supplements about which we have written before. He takes CoQ10, Turmeric, Nettle Root, sublingual Glutathione, vitamin B complex, a multivitamin with almost no iron or other heavy metals, slippery elm and fenugreek and a few others. Some of them are obviously helping. For one month we added a zinc ascorbate with vitamin C to help restore a bit of his sense of smell...which it has. He won't take that again for another month or two because taking for longer is contraindicated.
He also takes several supplements about which we have written before. He takes CoQ10, Turmeric, Nettle Root, sublingual Glutathione, vitamin B complex, a multivitamin with almost no iron or other heavy metals, slippery elm and fenugreek and a few others. Some of them are obviously helping. For one month we added a zinc ascorbate with vitamin C to help restore a bit of his sense of smell...which it has. He won't take that again for another month or two because taking for longer is contraindicated.
TOMORROW: The Questionnaire
Followed by: PD Tests - The progression scales
Subscribe to:
Posts (Atom)
PARKINSON'S FOCUS TODAY

A Top PD Blog award from Medical Transcriptions

We're among our favorite PD blogs - just click the badge to visit them. Click your back button to return.
Subscribe: Parkinson's Focus Today


Exercising

on the Total Gym
Tennis ball Hand Exercises -Stretching

To relieve stiffness: Insert ball between fingers as far as you can. Repeat between each finger. Stretching NOT squeezing is the important element of this exercise. Your goal is to prevent muscle tightening.
Yawning As Exercise

A full open-mouth yawn will open your throat - tilt your head back, yawn and feel what happens
ooo O aah A eee

A good exercise for doing in the morning and at night or anytime to open the throat and exercise those swallowing and speaking muscles
Posture and Gait as a symptom of PD
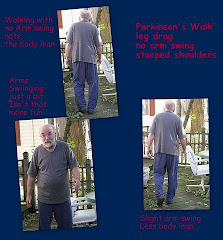
Lack of arm swing - foot drag - shoulder stoop - small stwps
Reflections

There is always hope
In Younger Days

Was the PD apparent then but we missed it?
A Tulip In Recognition of Parkinson's Disease

Innocence

Their Dad has PD